A nurse on the labor and delivery unit is planning care for a client who has human immunodeficiency virus (HIV). Which of the following is an appropriate action for the nurse to take following the birth of the newborn?
Cleanse the newborn immediately after delivery.
Initiate contact precautions for the newborn.
Administer intravenous antibiotics to the newborn.
Encourage the mother to breastfeed her newborn.
The Correct Answer is A
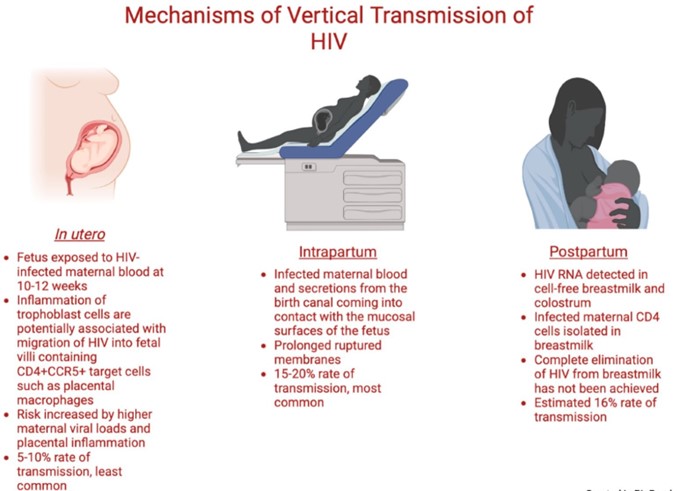
A newborn who is exposed to HIV perinatally should be bathed and cleansed of maternal secretions as soon as possible after birth to reduce the risk of HIV transmission through the skin or mucous membranes¹². The newborn should also receive antiretroviral prophylaxis within six hours of delivery, preferably within two hours¹². The type and duration of prophylaxis depend on the maternal and infant factors that influence the risk of HIV transmission, such as maternal viral load, antiretroviral therapy, mode of delivery, and infant gestational age¹²³. The newborn should also undergo HIV testing at birth, at 14 to 21 days of age, at one to two months of age, and at four to six months of age¹².
The other options are incorrect because:
b) Initiating contact precautions for the newborn is not necessary or recommended. Contact precautions are used to prevent the spread of infections that are transmited by direct or indirect contact with the patient or the patient's environment. HIV is not transmited by casual contact, and standard precautions are sufficient to prevent exposure to blood or body fluids that may contain HIV¹².
c) Administering intravenous antibiotics to the newborn is not indicated for HIV prevention. Antibiotics are used to treat bacterial infections, not viral infections like HIV. Antibiotics may be given to the newborn for other reasons, such as suspected sepsis or chorioamnionitis, but they do not affect the risk of HIV transmission¹².
d) Encouraging the mother to breastfeed her newborn is contraindicated for HIV prevention. Breastfeeding can transmit HIV from the mother to the infant through breast milk, especially if the mother has a high viral load, mastitis, cracked nipples, or oral lesions in the infant. In resource-limited settings where formula feeding may not be feasible or safe, breastfeeding with maternal or infant antiretroviral therapy may be considered, but in developed countries where safe alternatives are available, breastfeeding is not recommended for mothers with HIV infection¹².
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A spontaneous abortion (also called a miscarriage) is the unexpected ending of a pregnancy in the first 20 weeks of gestation. The major symptoms of a spontaneous abortion are abdominal cramps and bleeding from the vagina, sometimes with clots and/or bits of tissue³. A dilated cervix indicates that abortion is inevitable¹. Other symptoms may include low back ache, a decrease in pregnancy symptoms, and leaking amniotic fluid.
The other options are not answers because they are not indicative of an imminent spontaneous abortion.
b. Slight abdominal cramps
Slight abdominal cramps are a common symptom of early pregnancy and do not necessarily mean that a miscarriage is happening. However, if the cramps are severe, persistent, or accompanied by bleeding, then they could be a sign of a problem and should be reported to the provider.
c. Elevated hCG
hCG (human chorionic gonadotropin) is a hormone produced by the placenta during pregnancy. It can be measured in the blood or urine to confirm pregnancy or monitor its progress. Elevated hCG levels are not a sign of a spontaneous abortion, but rather a normal finding in early pregnancy. In fact, low or decreasing hCG levels may indicate a miscarriage or an ectopic pregnancy.
d. Scant bright red spotting
Scant bright red spotting is another common symptom of early pregnancy and does not necessarily mean that a miscarriage is happening. It may be caused by implantation bleeding, cervical irritation, or sexual intercourse. However, if the spotting is heavy, dark, or accompanied by cramps or pain, then it could be a sign of a problem and should be reported to the provider.
Correct Answer is D
Explanation
Heart rate is one of the vital signs that reflects the health and well-being of a newborn. It is measured by counting the number of heart beats per minute, either by listening to the chest with a stethoscope or by feeling the pulse at the wrist, elbow, or groin. Heart rate can vary depending on the newborn's activity level, temperature, and emotional state¹.
The normal range for heart rate in full-term newborns is 120 to 160 beats per minute. The heart rate may be slightly higher or lower depending on the newborn's age, weight, and gestational age. For example, premature newborns may have a higher heart rate than term newborns, and heavier newborns may have a lower heart rate than lighter newborns¹².
A heart rate that is too high (tachycardia) or too low (bradycardia) can indicate a problem with the newborn's heart function, oxygenation, or circulation. Some of the possible causes of abnormal heart rate in newborns are:
- Congenital heart defects: structural abnormalities of the heart that are present at birth and affect the blood flow through the heart and the body. They can cause cyanosis (bluish skin color), murmur (abnormal heart sound), poor feeding, or failure to thrive¹³.
- Arrhythmias: irregular or abnormal heart rhythms that can affect the electrical impulses that control the heartbeat. They can cause palpitations (feeling of skipped or extra beats), dizziness, fainting, or cardiac arrest¹³.
- Hypoxia: lack of oxygen in the blood or tissues that can affect the brain and other organs. It can be caused by respiratory distress, anemia, infection, or birth asphyxia. It can cause bradycardia, apnea (pauses in breathing), seizures, or coma¹⁴.
- Hypothermia: low body temperature that can affect the metabolism and organ function. It can be caused by exposure to cold environment, infection, or prematurity. It can cause bradycardia, lethargy, poor feeding, or hypoglycemia (low blood sugar)¹⁴.
- Sepsis: severe infection that can affect the whole body and cause inflammation and organ damage. It can be caused by bacteria, viruses, fungi, or parasites that enter the bloodstream from the mother, the umbilical cord, or the environment. It can cause tachycardia, fever, chills, poor feeding, or shock¹⁴.
Therefore, the nurse should report a heart rate of 72/min to the provider as an abnormal finding and monitor the newborn for any other signs of distress or illness. The provider may order further tests or treatments to determine the cause and severity of the low heart rate and prevent any complications.
The other findings are not findings that the nurse should report to the provider because they are within the
normal range for full-term newborns:
- a) Respiratory rate 55/min is within the normal range for respiratory rate in full-term newborns. The normal range for respiratory rate in full-term newborns is 40 to 60 breaths per minute. The respiratory rate may vary depending on the newborn's activity level, temperature and emotional state¹².
- b) Blood pressure 80/50 mm Hg is within the normal range for blood pressure in full-term newborns. The normal range for blood pressure in full-term newborns is 65 to 95 mm Hg for systolic pressure (the top number) and 30 to 60 mm Hg for diastolic pressure (the bottom number). The blood pressure may vary depending on the newborn's age, weight, and gestational age¹².
- c) Temperature 36.5°C (97.7°F) is within the normal range for temperature in full-term newborns. The normal range for temperature in full-term newborns is 36.5°C to 37.5°C (97.7°F to 99.5°F). The temperature may vary depending on the newborn's activity level, clothing, and environment¹².
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today