A patient has been admitted to the intensive care unit with cardiogenic shock and their blood pressure is 78/38. Which vasopressor medication is recognized as the first-line treatment for cardiogenic shock?
Dopamine
Norepinephrine
Epinephrine
Vasopressin (Pitressin)
The Correct Answer is B
Choice A rationale:
Dopamine is a catecholamine that acts on both alpha- and beta-adrenergic receptors. It has inotropic (increases heart contractility), chronotropic (increases heart rate), and vasopressor (constricts blood vessels) effects.
It was previously used as a first-line agent for cardiogenic shock, but it has fallen out of favor due to concerns about its potential to increase heart rate and arrhythmias, which can worsen myocardial oxygen demand and ischemia.
Additionally, dopamine's effects on renal blood flow can be unpredictable, and it may not be as effective as norepinephrine in increasing blood pressure in patients with severe shock.
Choice B rationale:
Norepinephrine is a potent alpha-adrenergic agonist that causes vasoconstriction, leading to an increase in blood pressure. It has minimal beta-adrenergic effects, so it does not significantly increase heart rate.
Norepinephrine is the preferred first-line vasopressor for cardiogenic shock because it effectively raises blood pressure without significantly increasing heart rate or myocardial oxygen demand.
It also has beneficial effects on renal blood flow and may improve organ perfusion.
Choice C rationale:
Epinephrine is a potent alpha- and beta-adrenergic agonist. It has strong inotropic, chronotropic, and vasopressor effects.
It can be used in cardiogenic shock, but it is typically reserved for patients who do not respond adequately to norepinephrine or who have severe bradycardia.
Epinephrine's potent beta-adrenergic effects can increase heart rate and myocardial oxygen demand, which can be detrimental in patients with cardiogenic shock.
Choice D rationale:
Vasopressin (Pitressin) is a hormone that acts on V1 receptors in vascular smooth muscle to cause vasoconstriction. It is not a first-line agent for cardiogenic shock, but it can be used as an adjunct to norepinephrine in patients who are refractory to other vasopressors.
Vasopressin may be particularly useful in patients with septic shock, as it has been shown to improve outcomes in this population.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","D"]
Explanation
Rationale for Choice A: Nitroglycerin IV gtt, titrate for SBP > 180mmHg
Mechanism of action: Nitroglycerin is a potent vasodilator that acts primarily on veins, but also has some arterial vasodilatory effects. It relaxes vascular smooth muscle by stimulating the production of nitric oxide, which causes vasodilation. This decrease in preload (venous return to the heart) and afterload (resistance against which the heart pumps) leads to a reduction in blood pressure.
Indications: Nitroglycerin is a preferred agent for hypertensive emergencies associated with acute heart failure, acute coronary syndromes, and aortic dissection. It is also effective in hypertensive emergencies with elevated intracranial pressure.
Dosage and administration: Nitroglycerin is typically administered as an intravenous infusion, starting at a low dose and titrating up based on blood pressure response. The goal is to titrate the medication to maintain systolic blood pressure below 180 mmHg.
Contraindications: Nitroglycerin is contraindicated in patients with a known hypersensitivity to nitrates, severe hypotension (systolic blood pressure < 90 mmHg), or those who have recently used phosphodiesterase-5 inhibitors (such as sildenafil).
Monitoring: During nitroglycerin infusion, it's essential to monitor blood pressure closely, as well as heart rate, for any signs of hypotension or tachycardia.
Rationale for Choice B: Labetalol (Normodyne) 10mg IVP q 10 minutes prn for SBP >170 mmHg
Mechanism of action: Labetalol is a mixed alpha- and beta-adrenergic blocker. It blocks the effects of norepinephrine and epinephrine, leading to vasodilation and a decrease in heart rate.
Indications: Labetalol is a versatile agent that can be used in various hypertensive emergencies, including those associated with acute aortic dissection, acute coronary syndromes, and pre-eclampsia/eclampsia. It's also useful in patients with a history of asthma or chronic obstructive pulmonary disease (COPD), as it has less bronchoconstrictive effects than beta-blockers like propranolol.
Dosage and administration: Labetalol can be administered as an intravenous bolus or infusion. In this scenario, it's prescribed as a 10mg intravenous push every 10 minutes as needed for systolic blood pressure greater than 170 mmHg.
Contraindications: Labetalol is contraindicated in patients with severe bradycardia, heart block, cardiogenic shock, or decompensated heart failure.
Monitoring: During labetalol administration, it's important to monitor blood pressure, heart rate, and electrocardiogram (ECG) for any signs of bradycardia, heart block, or other arrythmias.
Rationale for Choice D: Nitroprusside (Nitropress) IV gtt titrate to keep SBP < 160 mmHg
Mechanism of action: Nitroprusside is a potent vasodilator that acts directly on both arterioles and veins. It relaxes vascular smooth muscle by releasing nitric oxide, leading to a rapid and profound decrease in blood pressure.
Indications: Nitroprusside is often reserved for hypertensive emergencies that are refractory to other agents or those that require rapid blood pressure control, such as hypertensive encephalopathy or acute aortic dissection.
Dosage and administration: Nitroprusside is administered as an intravenous infusion and titrated to the desired blood pressure response. The goal is to keep systolic blood pressure below 160 mmHg.
Contraindications: Nitroprusside is contraindicated in patients with severe renal impairment or those with increased intracranial pressure.
Monitoring: Nitroprusside therapy requires close monitoring of blood pressure, as well as monitoring for thiocyanate toxicity (a metabolite of nitroprusside) in patients with prolonged infusion or renal impairment.
Correct Answer is D
Explanation
Choice A rationale:
Stevens-Johnson syndrome (SJS) is a rare, serious skin condition that is typically caused by an allergic reaction to medication. While amiodarone has been associated with a few cases of SJS, it is not considered a common long-term side effect.
Choice B rationale:
Ventricular tachycardia (VT) is a type of fast heart rhythm that originates in the ventricles of the heart. Amiodarone is actually used to treat VT, so it would be counterintuitive to list it as a long-term side effect.
Choice C rationale:
Pulmonary fibrosis is a condition characterized by scarring of the lung tissue. While amiodarone can cause pulmonary toxicity, which includes pulmonary fibrosis, this is a relatively rare side effect. Moreover, it's usually associated with high doses or
long-term use of the medication.
Choice D rationale:
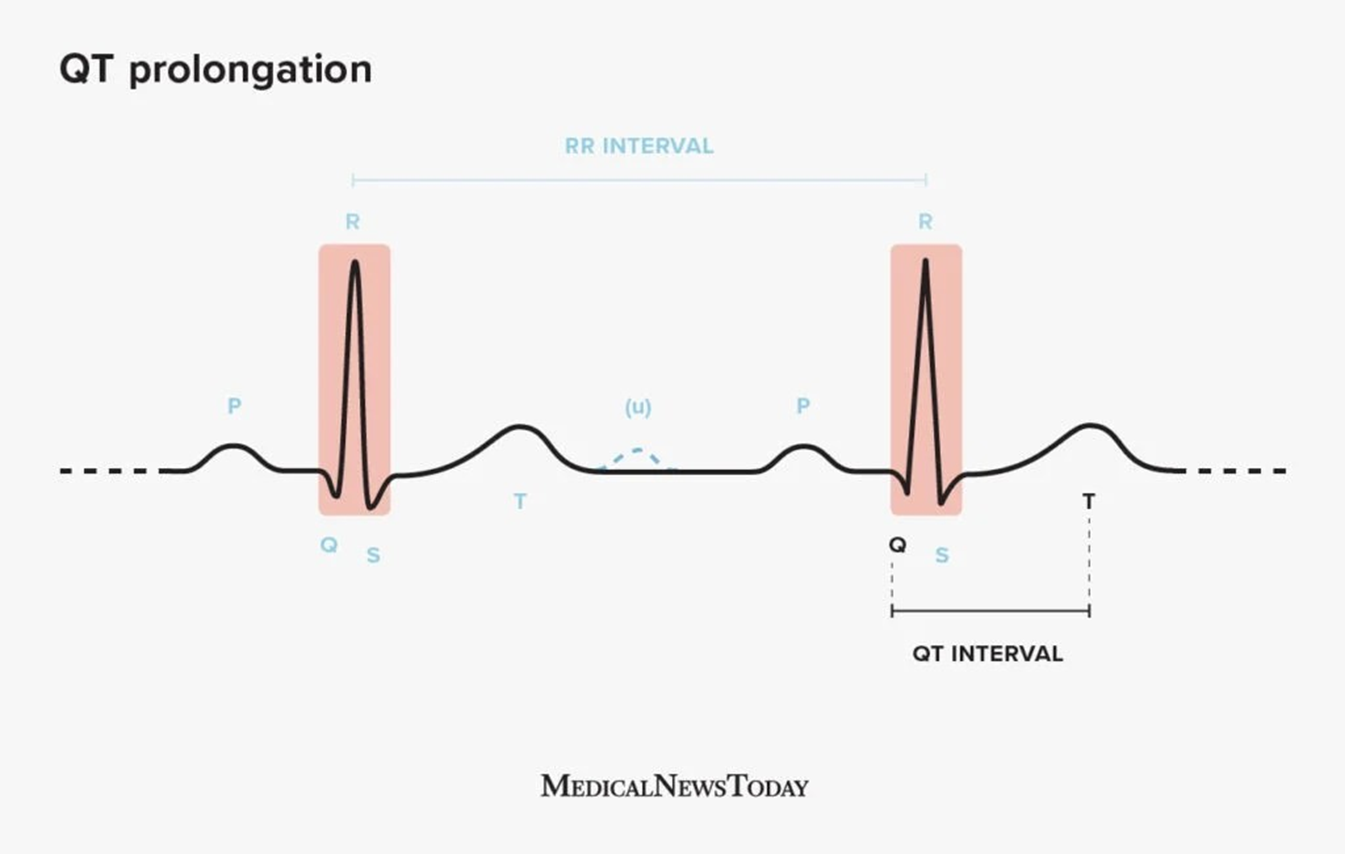
QT prolongation is a condition in which the heart's electrical activity takes longer than normal to recharge between beats. This can lead to a potentially fatal arrhythmia called torsades de pointes. Amiodarone is known to prolong the QT interval, and this is considered one of its most significant long-term side effects. It's important to monitor patients on amiodarone for QT prolongation and to adjust the dose or discontinue the medication if necessary.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today