A school nurse is performing scoliosis screenings. The nurse should recognize which of the following clinical manifestations as an indication of scoliosis?
Mild pain at the hip region
Uneven shoulder and pelvic heights
Limited range of motion of hips
Exaggerated curvature of the sacrum
The Correct Answer is B
Choice A reason:
Mild pain in the hip region can be caused by various musculoskeletal issues, such as muscle strains, bursitis, or even referred pain from other areas. It is not a characteristic symptom of scoliosis.
Choice B reason
Scoliosis is characterized by an abnormal sideways curvature of the spine, which can cause uneven shoulders and pelvic heights. As the spine curves abnormally, it can lead to asymmetry in the shoulders and hips, which are noticeable during physical examination. This asymmetry is a key clinical sign that suggests the presence of scoliosis.
Choice C reason:
Limited range of motion (ROM) of the hips is more likely related to hip joint issues or musculoskeletal conditions affecting the hips, not specifically scoliosis.
Choice D reason:
Exaggerated curvature of the sacrum may indicate other spinal abnormalities or conditions affecting the lower back, but it is not typically associated with scoliosis, which primarily affects the curvature of the spine higher up in the thoracic or lumbar regions.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. This choice is correct because a child who has autism spectrum disorder often exhibits strict adherence to routines and rituals, and may become distressed or agitated when there are changes or disruptions to their usual patterns.
B. This choice is incorrect because difficulty paying attention to tasks is not a specific manifestation of autism spectrum disorder, but rather a common symptom of attention-deficit/hyperactivity disorder (ADHD). A child who has autism spectrum disorder may have difficulty focusing on tasks that are not of interest to them, but may also show intense concentration on tasks that are of interest to them.
C. This choice is incorrect because disobedience to authority figures is not a specific manifestation of autism spectrum disorder, but rather a common behavior problem in children and adolescents. A child who has autism spectrum disorder may have difficulty understanding social cues and expectations, but may also show compliance and cooperation when given clear instructions and positive reinforcement.
D. This choice is incorrect because excessive anxiety when separated from parents is not a specific manifestation of autism spectrum disorder, but rather a common symptom of separation anxiety disorder. A child who has autism spectrum disorder may have difficulty forming attachments and expressing emotions, but may also show affection and attachment to familiar people.
Correct Answer is B
Explanation
Choice A reason
While thinning of secretions can be a positive sign, it's not always visible. A decrease in peak inspiratory pressure is a more objective indicator of improved airway patency.
Choice B reason.
Peak inspiratory pressure is the maximum pressure required to push air into the lungs. If suctioning is effective, it will remove secretions and reduce airway resistance, leading to a decrease in peak inspiratory pressure.
Choice C reason:
While a productive cough can indicate that secretions are being moved, it doesn't directly measure the effectiveness of suctioning.
Choice D reason:
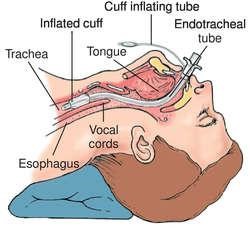
Flattening of the artificial airway cuff: Flattening of the artificial airway cuff is not a relevant indicator of the effectiveness of suctioning. The cuff of an endotracheal tube is inflated to prevent air leaks around the tube and to maintain proper ventilation. It is not directly related to the effectiveness of suctioning.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today