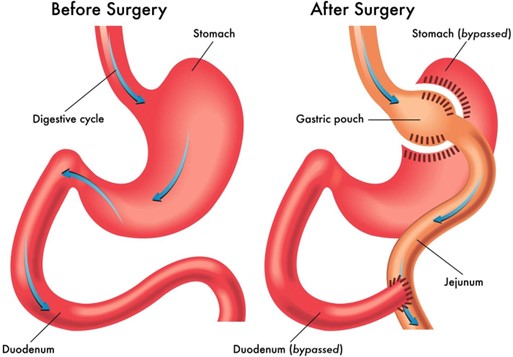
An adult woman who had gastric bypass surgery two weeks ago is admitted because she is exhibiting signs of anastomosis leakage. Her vital signs are: temperature 100°F (37.8°C), blood pressure 98/50 mm Hg, heart rate 135 beats/minute, and respiratory rate 24 breaths/minute. Which intervention is most important for the nurse to include in this client's plan of care?
Replace fluids intravenously based on intake and output.
Record the amount of daily wound drainage.
Assess skin condition and turgor for breakdown.
Turn every 2 hours around the clock from side-to-side.
The Correct Answer is A
Choice A Reason: This is the correct answer because the client's vital signs indicate that she is hypovolemic and dehydrated due to the leakage of gastric contents from the anastomosis site. The nurse should replace fluids intravenously to prevent shock and electrolyte imbalance.
Choice B Reason: Recording the amount of daily wound drainage is important but not the most important intervention for this client because it does not address the immediate problem of fluid loss and hypovolemia. The nurse should monitor the wound drainage for signs of infection and report any changes to the physician.
Choice C Reason: Assessing skin condition and turgor for breakdown is important but not the most important intervention for this client because it does not address the immediate problem of fluid loss and hypovolemia. The nurse should assess the skin for signs of dehydration and pressure ulcers and provide appropriate skin care.
Choice D Reason: Turning every 2 hours around the clock from side-to-side is important but not the most important intervention for this client because it does not address the immediate problem of fluid loss and hypovolemia. The nurse should turn the client to prevent complications such as pneumonia and atelectasis but also consider the client's comfort and pain level.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: Ensuring the transfer of the client's electronic chart code is not the most important action for the nurse to take first. The electronic chart code is a unique identifier that allows access to the client's health records and care plan. While this is an important task, it is not as urgent or essential as giving a detailed report to the accepting nurse, who will be responsible for providing palliative care to the client.
Choice B Reason: Giving a detailed report to the accepting nurse is the most important action for the nurse to take first. The report should include the client's diagnosis, prognosis, pain level, medication regimen, preferences, goals, and psychosocial needs. This will ensure continuity of care and facilitate a smooth transition for the client and the family.
Choice C Reason: Taking the family to the client's new room is not the most important action for the nurse to take first. The family may need emotional support and guidance during this difficult time, but they also need accurate and timely information about the client's condition and care plan. The nurse should first give a detailed report to the accepting nurse and then accompany the family to the new room.
Choice D Reason: Giving the client written information about end-of-life care is not the most important action for the nurse to take first. The client may benefit from learning more about palliative care, hospice care, advance directives, and bereavement services, but this should be done after giving a detailed report to the accepting nurse and ensuring that the client is comfortable and stable in the new room.
Correct Answer is A
Explanation
Choice A Reason: This client has a very high BNP level, which indicates severe heart failure and fluid overload. The nurse should follow up with this client first, as they may need urgent interventions such as oxygen therapy, diuretics, and vasodilators.
Choice B Reason: This client has an INR within the therapeutic range for warfarin therapy, which is usually between 2 and 3. The nurse should monitor this client for signs of bleeding or clotting, but they do not require immediate follow-up.
Choice C Reason: This client has a mildly elevated glucose level, which may be caused by the corticosteroids that
increase blood sugar. The nurse should check the client's blood glucose regularly and administer insulin as ordered, but they do not require immediate follow-up.
Choice D Reason: This client has a normal potassium level, which is within the reference range of 3.5 to 5 mEq/L. The nurse should ensure that the client is ready for dialysis and avoid foods high in potassium, but they do not require immediate follow-up.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today