Aureissisting a nurse midwife in examining a client who is a primigravida at 42 weeks of gestation and states that she thinks she is in labor. Which of the following findings confirms that the client is in labor?
Fain just above the navel
Cervical dilation
Amniotic fluid in the vaginal vault
Contractions every 3 to 4 min
The Correct Answer is B
Choice A rationale: Pain above the navel is not a specific indicator of labor and may be unrelated to the onset of labor.
Choice B rationale: Cervical dilation is a definitive sign of labor. It indicates that the cervix is opening to allow the baby's passage through the birth canal.
Choice C rationale: The presence of amniotic fluid in the vaginal vault (rupture of membranes) could indicate that the client's water has broken, but it does not confirm active labor. Labor can begin before or after the rupture of membranes.
Choice D rationale: Regular contractions are a typical sign of labor, but their frequency alone does not confirm active labor. Other signs, such as cervical dilation and effacement, are necessary to confirm active labor.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A rationale:
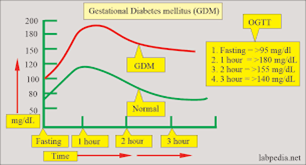
A 3-hour oral glucose tolerance test is typically done during the initial diagnosis of gestational diabetes, not for ongoing monitoring. Since the client is already diagnosed, this action is not necessary at this stage.
Choice B rationale:
Obtaining an HbA1C is not necessary in this situation. HbA1C provides information about average blood glucose levels over the past 2-3 months and is not specific to postprandial glucose levels.
Choice C rationale:
Telling the client to increase carbohydrates to 65% of daily nutritional intake would not be appropriate since the client already has elevated blood glucose levels. Reducing carbohydrate intake and focusing on a balanced diet are more appropriate for managing gestational diabetes.
Choice D rationale:
Given that the client's blood glucose levels after meals are consistently above the target range (generally <140 mg/dL for 1-hour post-meal), it indicates a need for better glycemic control, which may require insulin therapy.
Correct Answer is ["A","B","C"]
Explanation
Choice A rationale: The Scarf sign assesses the range of motion of the newborn's shoulder and elbow joint. It measures the ability of the newborn's arm to be brought across the chest.
Choice B rationale: Arm recoil measures the degree of resistance and recoil of the newborn's arm when it is extended and then flexed against the chest. This reflex provides information about the newborn's muscle tone and neuromuscular maturity.
Choice C rationale: The Moro reflex, also known as the startle reflex, is elicited by a sudden change in the newborn's position or by a loud noise. It involves an initial extension and abduction of the arms, followed by a flexion and adduction. This reflex helps assess the newborn's neurologic and neuromuscular maturity.
Choice D rationale: "Heel to ear" is not a standard neuromuscular assessment used in the gestational age assessment. It may be an incorrect or unclear term.
Choice E rationale: The popliteal angle is not a neuromuscular assessment used in the gestational age assessment. It measures the angle of flexion in the knee joint and is not directly related to neuromuscular maturity
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today