A nurse is reviewing laboratory results from a client who is at 28 weeks of gestation and has gestational diabetes. The nurse notes that blood glucose levels taken 1 hr following a meal range from 145 mg/dL to 162 mg/dL over the past week. Which of the following actions should the nurse take?
Schedule a 3-hr oral glucose tolerance test.
Tell the client to increase carbohydrates to 65% of daily nutritional intake.
Obtain an HbA1c.
Reinforce instruction about insulin administration.
The Correct Answer is D
Choice A rationale:
The nurse should schedule a 3-hour oral glucose tolerance test (OGTT) for the client because the blood glucose levels taken 1 hour following a meal are higher than the expected range for gestational diabetes. This test will help to diagnose and assess the client's glucose tolerance and determine if there is gestational diabetes or any other potential glucose regulation issues.
Choice B rationale:
Increasing carbohydrates to 65% of daily nutritional intake is not the appropriate action in this situation. It may lead to further elevation of blood glucose levels, which can be detrimental for a client with gestational diabetes. The goal is to manage blood glucose levels and prevent complications, so recommending a higher carbohydrate intake would be counterproductive.
Choice C rationale:
Obtaining an HbA1c (glycated hemoglobin) is not the most suitable action in this scenario. HbA1c provides an average of the blood glucose levels over the past few months, which is more helpful for diagnosing and monitoring chronic diabetes, rather than gestational diabetes, which is temporary and occurs during pregnancy. An OGTT is a more appropriate test for gestational diabetes assessment.
Choice D rationale:
Reinforcing instruction about insulin administration is not warranted at this point since there is no information indicating that the client is currently on insulin therapy. Additionally, using insulin as the first step in the management of gestational diabetes is not common practice. Lifestyle modifications, dietary changes, and other measures are usually attempted first.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
The correct answer is choice A, Maternal hypertension.
Choice A rationale:
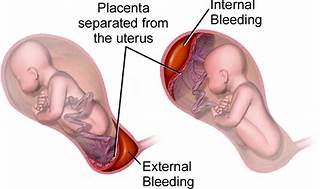
Maternal hypertension is widely recognized as the most common risk factor for placental abruption. High blood pressure can cause the placenta to detach from the uterine wall, leading to abruption. In summary, while all the listed factors can contribute to the risk of placental abruption, maternal hypertension stands out as the most common cause, supported by multiple health sources. It’s important for nurses to recognize and manage hypertension in pregnant clients to minimize the risk of this serious complication.
Choice B rationale:
While maternal cocaine use is a significant risk factor for placental abruption due to its vasoconstrictive effects, which can compromise the placental blood flow, it is not as common as maternal hypertension.
Choice C rationale:
Maternal cigarette smoking is also a risk factor for placental abruption. Smoking can lead to a variety of complications in pregnancy, including placental problems, but again, it is less common than hypertension as a cause for abruption.
Choice D rationale:
Maternal battering can lead to trauma which may result in placental abruption. However, it is not considered the most common risk factor when compared to maternal hypertension.
Correct Answer is A
Explanation
Step 1 is assessing heart rate. A heart rate of 130/min earns 2 points since a rate above 100/min is optimal.
Step 2 is assessing respiratory effort. A lusty cry earns 2 points as strong crying indicates good respiratory function.
Step 3 is assessing muscle tone. Flexed extremities earn 1 point since full active movement would score 2.
Step 4 is assessing reflex irritability. Grimace when suctioned earns 1 point as a vigorous response (cough, sneeze) would score 2.
Step 5 is assessing color. Acrocyanosis earns 1 point since a fully pink body scores 2.
Final answer: 7
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today