In caring for a client who is receiving meropenem IV for nosocomial pneumonia, which assessment finding is most important for the nurse to report to the health care provider?
Yellow-tinged sputum
Nausea and headache
Watery diarrhea
Increased fatigue
The Correct Answer is C
Choice A reason: Yellow-tinged sputum is not a critical finding for the nurse to report, as this is a common sign of pneumonia and does not indicate an adverse reaction to meropenem. This is a distractor choice.
Choice B reason: Nausea and headache are not urgent findings for the nurse to report, as these are mild side effects of meropenem and can be managed with supportive measures. This is another distractor choice.
Choice C reason: Watery diarrhea is an important finding for the nurse to report, as this can indicate a serious complication of meropenem, such as Clostridioides difficile infection, which can cause severe dehydration, electrolyte imbalance, and sepsis. Therefore, this is the correct choice.
Choice D reason: Increased fatigue is not a significant finding for the nurse to report, as this can be related to the client's underlying condition and does not suggest a problem with meropenem. This is another distractor choice.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
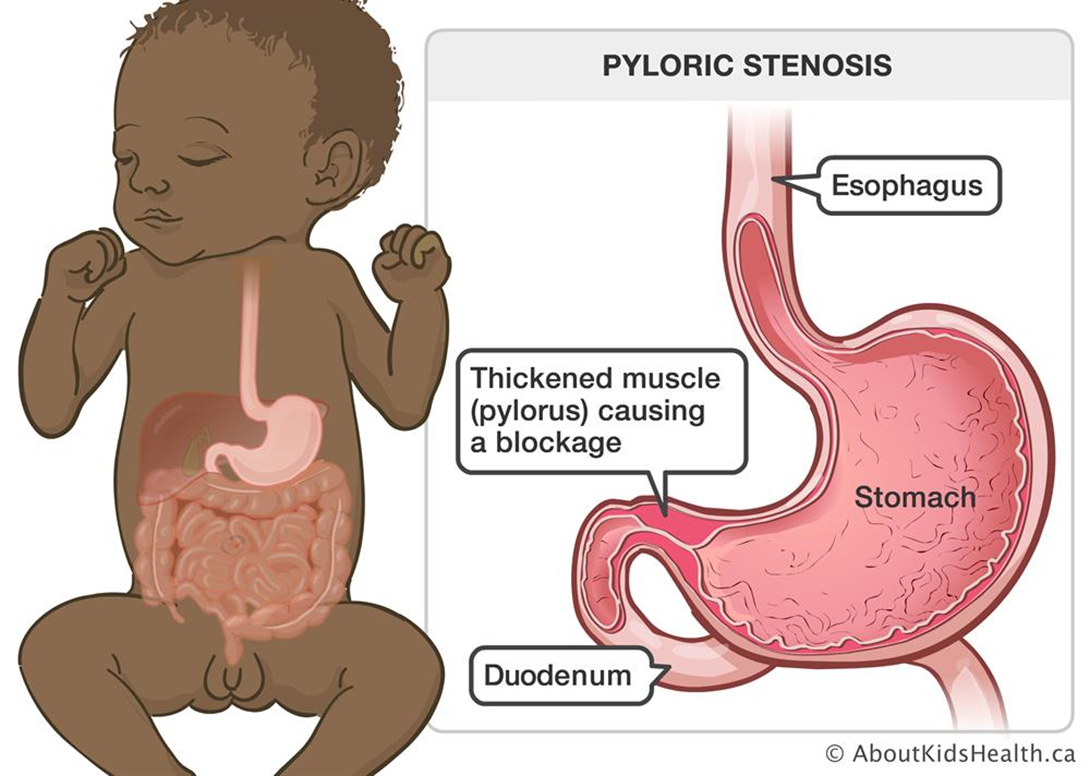
Choice A reason: Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
Choice B reason: Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.
Choice C reason: Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.
Choice D reason: This is the correct answer because initiating a continuous infusion of IV fluids per prescription is essential to prevent dehydration and electrolyte imbalance in the infant. The infant may have significant fluid loss due to vomiting and poor intake.
Correct Answer is C
Explanation
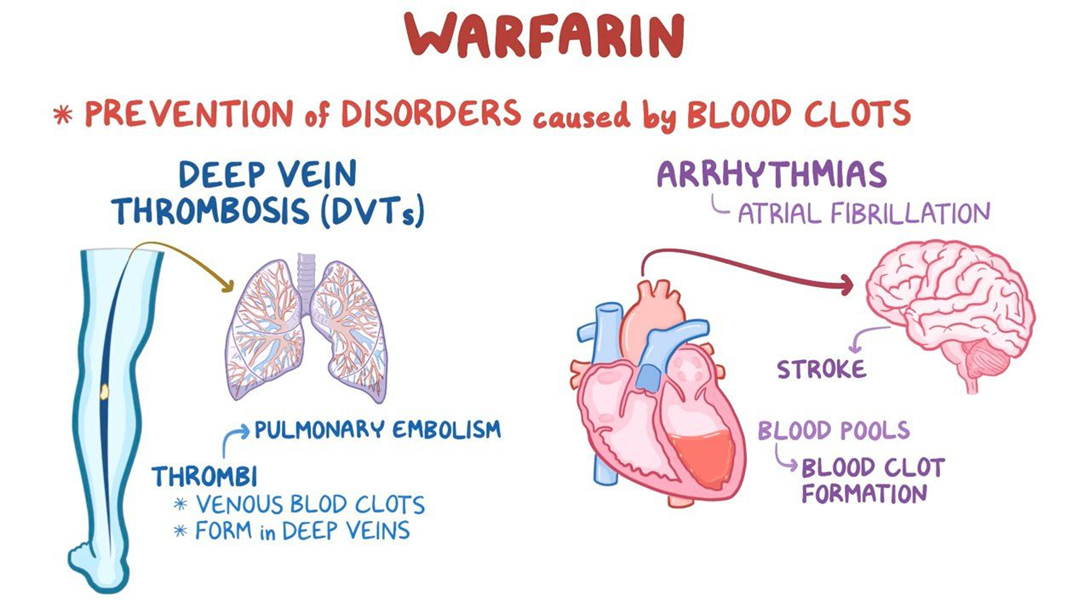
Choice A reason: Increasing the intake of dark green leafy vegetables while taking warfarin is not a good instruction because it can decrease the effectiveness of warfarin. Dark green leafy vegetables are rich in vitamin K, which is a coagulation factor that counteracts the anticoagulant effect of warfarin.
Choice B reason: Eating two servings of dark green leafy vegetables daily and continuing for 30 days after warfarin therapy is completed is not a good instruction because it can cause bleeding complications. Dark green leafy vegetables are rich in vitamin K, which is a coagulation factor that counteracts the anticoagulant effect of warfarin. Stopping warfarin while continuing to eat high amounts of vitamin K can increase the risk of clot formation and thromboembolism.
Choice C reason: This is the correct answer because eating approximately the same amount of leafy green vegetables daily so the amount of vitamin K consumed is consistent is a good instruction because it can help maintain a stable therapeutic level of warfarin. Dark green leafy vegetables are rich in vitamin K, which is a coagulation factor that counteracts the anticoagulant effect of warfarin. Keeping a consistent intake of vitamin K can help avoid fluctuations in warfarin's effect and prevent bleeding or clotting episodes.
Choice D reason: Avoiding eating any foods that contain any vitamin K because it is an antagonist of warfarin is not a good instruction because it can cause bleeding complications. Dark green leafy vegetables are rich in vitamin K, which is a coagulation factor that counteracts the anticoagulant effect of warfarin. Eliminating vitamin K from the diet can increase the sensitivity to warfarin and cause excessive bleeding and bruising.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today