The nurse is caring for a group of clients with the help of a practical nurse (PN). Which nursing action(s) should the nurse assign to the PN? (Select all that apply)
Obtain postoperative vital signs for a client one day following unilateral knee arthroplasty.
Perform daily surgical dressing change for a client who had an abdominal hysterectomy.
Initiate patient controlled analgesia (PCA. pumps for two clients immediately postoperatively.
Start the second blood transfusion for a client twelve hours following a below knee amputation.
Monitor a dose of warfarin per protocol for a client with type 2 diabetes mellitus (DM).
Correct Answer : A,B,E
Choice C reason: Initiating patient controlled analgesia (PCA. pumps for two clients immediately postoperatively is not a nursing action that can be assigned to the PN. PCA pump is a device that allows the client to self-administer pain medication through an IV line by pressing a button. PCA pump should be initiated by the nurse after verifying the prescription, setting the parameters, educating the client, and ensuring safety and effectiveness. The PN does not have the authority or competency to initiate PCA pump or adjust its settings.
Choice D reason: Starting the second blood transfusion for a client twelve hours following a below knee amputation is not a nursing action that can be assigned to the PN. Blood transfusion is a procedure that delivers donated blood or blood products into the client's bloodstream through an IV line. Blood transfusion should be started by the nurse after verifying the prescription, checking the blood type and compatibility, obtaining informed consent, and monitoring for any adverse reactions. The PN does not have the authority or competency to start blood transfusion or manage its complications.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: Notifying the healthcare provider is an important action, but not the first one. The nurse should prioritize interventions that address the client's immediate needs, such as oxygenation and circulation.
Choice B reason: Preparing a continuous heparin infusion per protocol is an appropriate action for preventing further clot formation and reducing the risk of recurrent pulmonary embolism, but it is not the first action. The nurse should first stabilize the client's condition before administering anticoagulant therapy.
Choice D reason: Bringing the emergency crash cart to the bedside is a prudent action, but not the first one. The nurse should prepare for possible cardiopulmonary resuscitation (CPR) in case of cardiac arrest, but should first attempt to prevent it by providing oxygen and other supportive measures.
Correct Answer is A
Explanation
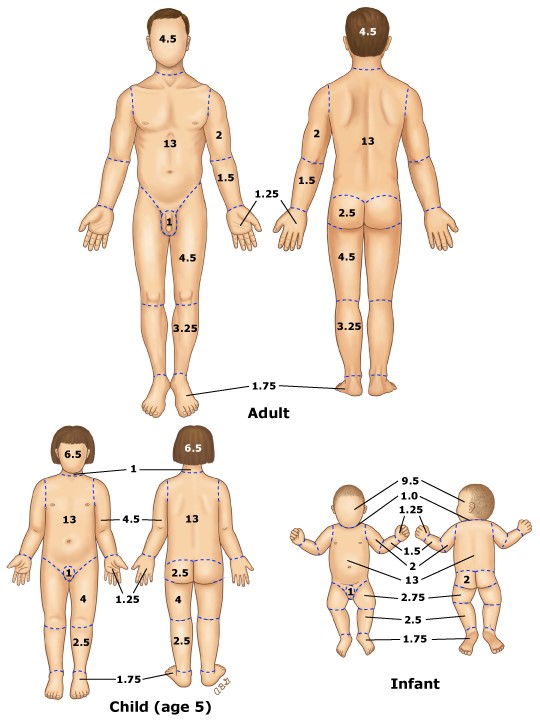
Choice A reason: This is the correct answer.According to the rule of nines, each leg accounts for 18% of the total body surface area, and the anterior surface of each leg accounts for half of that, or 9%. Therefore, the patient has partial-thickness burns on 9% + 9% = 18% of the body surface area.
Choice B reason: This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior and posterior surfaces of both legs, as well as the head and neck, which is not given in the question.
Choice C reason: This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior surface of only one leg, which is not given in the question.
Choice D reason: This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior and posterior surfaces of both legs, which is not given in the question.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today