A wound has a bloodtinged liquid that is dripping from the surgical site. How does the nurse document this finding?
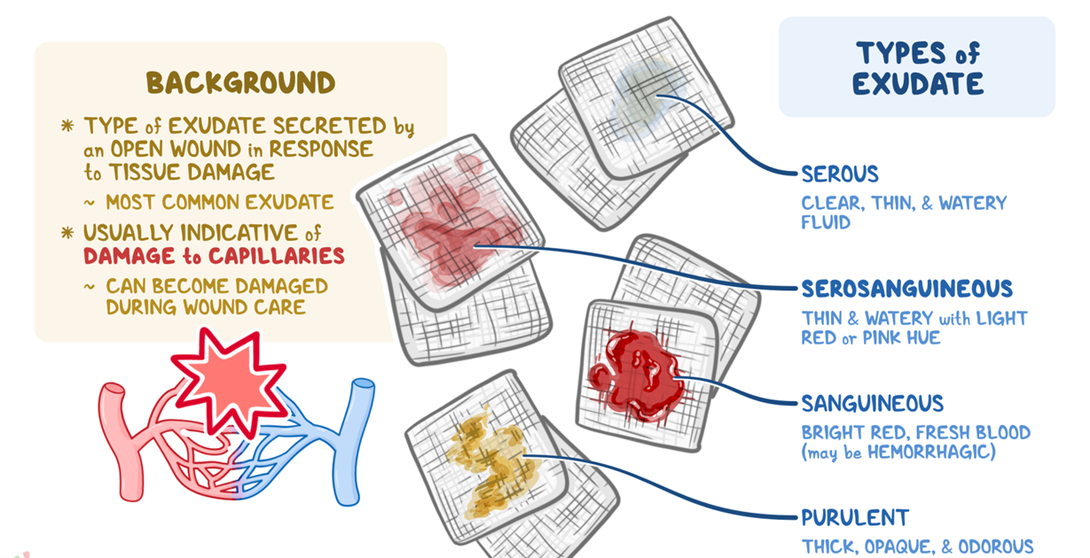
Purulent exudate
Serous exudate
Serosanguineous exudate
Sanguineous exudate
The Correct Answer is C
Choice A reason: Purulent exudate is a thick, yellowgreen, or brown pus that indicates infection. It is not bloodtinged and does not drip from the wound.
Choice B reason: Serous exudate is a clear, thin, and watery fluid that is normal in the inflammatory stage of wound healing. It does not contain blood cells and is not red in color.
Choice C reason: Serosanguineous exudate is a pink or red fluid that contains both serum and blood. It is common in the proliferative stage of wound healing and may drip from the wound due to increased capillary permeability.
Choice D reason: Sanguineous exudate is a bright or dark red fluid that consists mostly of blood. It indicates active bleeding and is usually seen in traumatic or surgical wounds. It is not diluted with serum and is more viscous than serosanguineous exudate.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: Nociceptive pain is not the type of pain that the client is experiencing. Nociceptive pain is caused by the stimulation of nociceptors, which are sensory receptors that detect tissue damage or potential harm. Nociceptive pain is usually localized, sharp, throbbing, or aching. It is associated with injuries such as cuts, burns, sprains, or fractures. The client's pain is not caused by any tissue damage or harm in the distal part of the amputated limb, as there is no tissue left there.
Choice B reason: Neuropathic pain is the type of pain that the client is experiencing. Neuropathic pain is caused by the damage or dysfunction of the nervous system, such as the peripheral nerves, the spinal cord, or the brain. Neuropathic pain is usually chronic, burning, shooting, or tingling. It is associated with conditions such as diabetes, shingles, stroke, or amputation. The client's pain is caused by the disruption of the nerve signals from the amputated limb, which creates a phantom sensation of pain in the missing part.
Choice C reason: Cutaneous pain is not the type of pain that the client is experiencing. Cutaneous pain is caused by the stimulation of the cutaneous receptors, which are sensory receptors that detect touch, temperature, or pressure on the skin. Cutaneous pain is usually superficial, brief, or pricking. It is associated with stimuli such as pinching, scratching, or cold. The client's pain is not caused by any touch, temperature, or pressure on the skin of the distal part of the amputated limb, as there is no skin left there.
Choice D reason: Visceral pain is not the type of pain that the client is experiencing. Visceral pain is caused by the stimulation of the visceral receptors, which are sensory receptors that detect stretch, inflammation, or ischemia in the internal organs. Visceral pain is usually deep, dull, or cramping. It is associated with conditions such as appendicitis, pancreatitis, or bowel obstruction. The client's pain is not caused by any stretch, inflammation, or ischemia in the internal organs of the distal part of the amputated limb, as there are no organs left there.
Correct Answer is C
Explanation
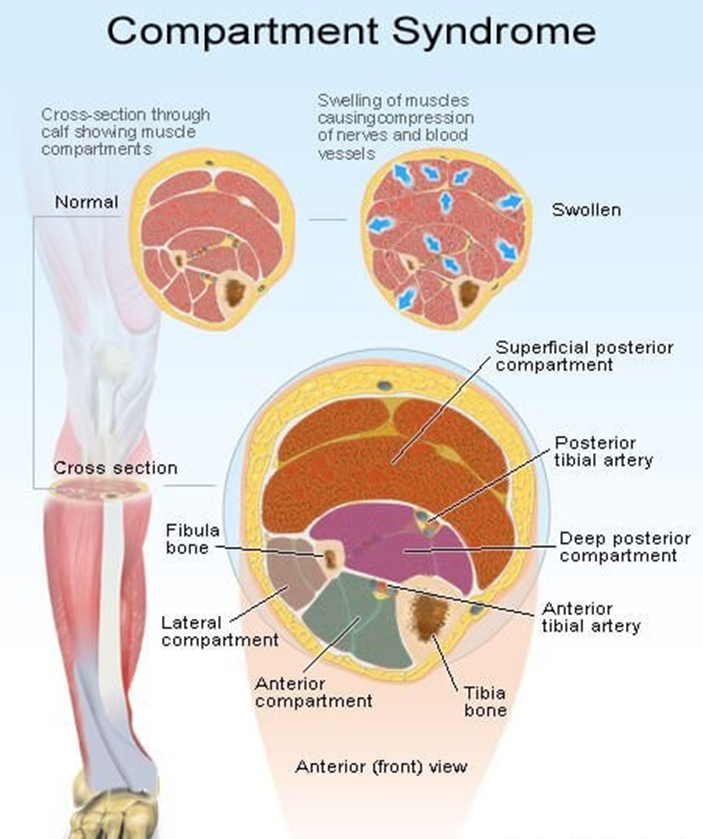
Choice A reason: A bone fragment has injured the nerve supply in the area is not the best response by the nurse. This may be a possible complication of a fracture, but it does not explain the mechanism of compartment syndrome. Compartment syndrome is a condition where the pressure within a closed space (such as a muscle compartment) exceeds the perfusion pressure and causes ischemia and necrosis of the tissues. A bone fragment may damage the nerve, but it does not cause increased pressure in the compartment.
Choice B reason: An injured artery causes impaired arterial perfusion through the compartment is not the best response by the nurse. This may be a possible cause of compartment syndrome, but it is not the most common one. Compartment syndrome is more often caused by venous obstruction than arterial obstruction. An injured artery may reduce the blood flow to the compartment, but it does not cause increased pressure in the compartment.
Choice C reason: Bleeding and swelling cause increased pressure in an area that cannot expand is the best response by the nurse. This is the most common cause of compartment syndrome and explains the pathophysiology of the condition. Bleeding and swelling are the result of inflammation and tissue injury that occur after a fracture. They increase the volume of fluid in the compartment, which cannot expand due to the rigid fascia that surrounds it. This leads to increased pressure in the compartment, which compresses the blood vessels, nerves, and muscles and causes ischemia and necrosis of the tissues.
Choice D reason: The fascia expands with injury, causing pressure on underlying nerves and muscles is not the best response by the nurse. This is not a correct statement, as the fascia does not expand with injury. The fascia is a tough connective tissue that encloses the muscle compartments and limits their expansion. The fascia is part of the problem, not the cause, of compartment syndrome. The fascia prevents the compartment from accommodating the increased volume of fluid and causes increased pressure in the compartment.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today