During a skin inspection at the outpatient clinic, the nurse notices patches of thick, red skin with silvery scales on the client's elbows and knees. What skin abnormality does the nurse suspect?
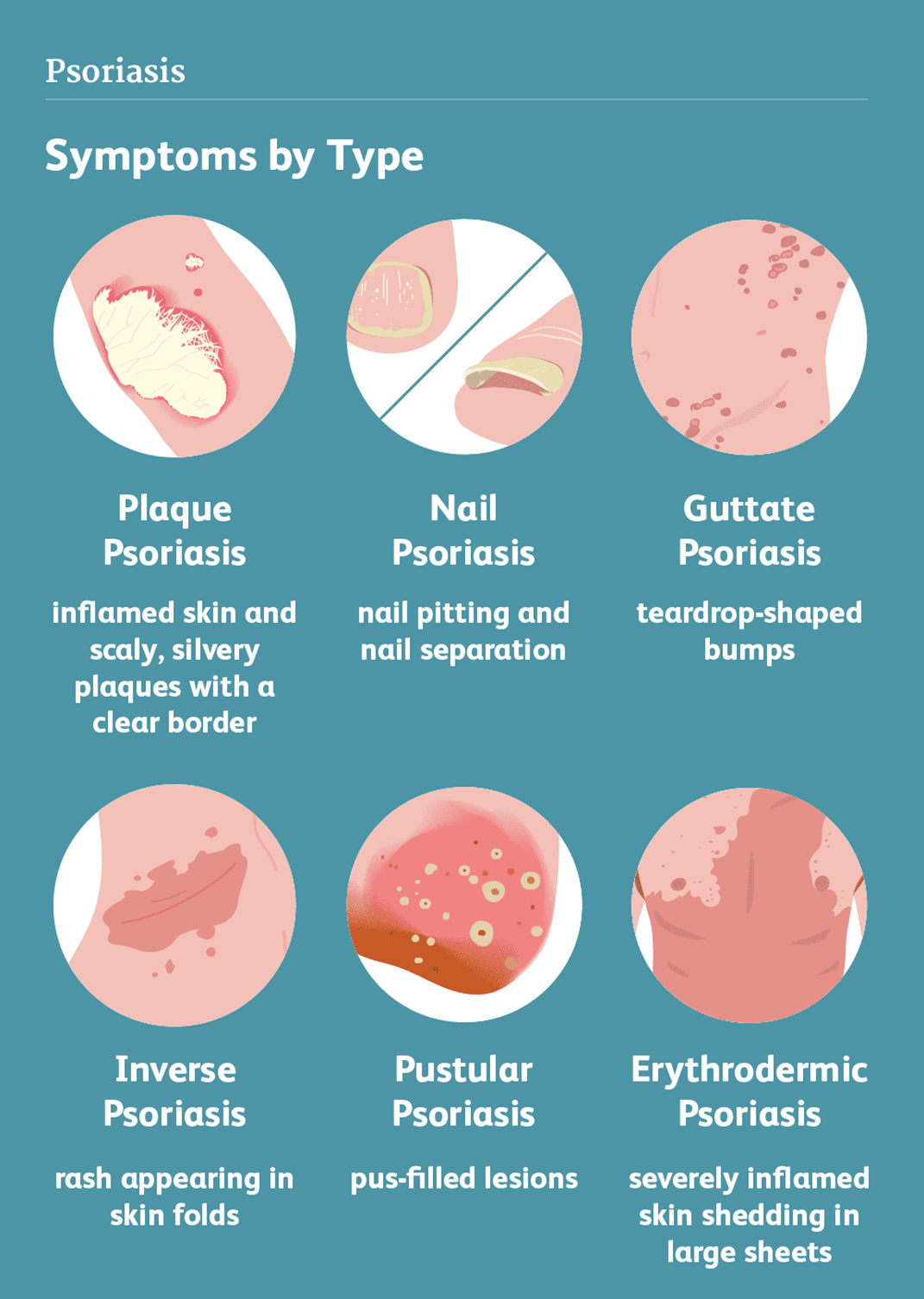
Psoriasis
Rosacea
Scabies
Stasis dermatitis
The Correct Answer is A
Choice A reason: Psoriasis is a skin abnormality that causes patches of thick, red skin with silvery scales, usually on the elbows, knees, scalp, lower back, or genitals. Psoriasis is a chronic, inflammatory, autoimmune condition that affects the life cycle of skin cells, causing them to build up rapidly on the surface of the skin. Psoriasis can cause itching, burning, pain, or bleeding.
Choice B reason: Rosacea is a skin abnormality that causes redness, flushing, swelling, or pimples, usually on the face, especially the cheeks, nose, chin, or forehead. Rosacea is a chronic, inflammatory, vascular condition that affects the blood vessels and sebaceous glands of the skin. Rosacea can cause sensitivity, stinging, or dryness.
Choice C reason: Scabies is a skin abnormality that causes small, red bumps, blisters, or burrows, usually on the hands, wrists, feet, ankles, or genitals. Scabies is a contagious, parasitic infection that is caused by tiny mites that burrow into the skin and lay eggs. Scabies can cause intense itching, especially at night.
Choice D reason: Stasis dermatitis is a skin abnormality that causes swelling, redness, scaling, or ulcers, usually on the lower legs or ankles. Stasis dermatitis is a chronic, inflammatory condition that results from poor blood circulation in the veins of the legs, causing fluid to leak into the surrounding tissues. Stasis dermatitis can cause pain, itching, or infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: A decreased level of rheumatoid factor is not seen in clients with rheumatoid arthritis. Rheumatoid factor is an antibody that is produced by the immune system and can bind to other antibodies. A high level of rheumatoid factor indicates an autoimmune disorder, such as rheumatoid arthritis.
Choice B reason: A negative rheumatoid factor is not seen in clients with rheumatoid arthritis. A negative rheumatoid factor means that the antibody is not detected in the blood. A negative rheumatoid factor does not rule out rheumatoid arthritis, but it may suggest a different type of arthritis or another condition.
Choice C reason: A positive rheumatoid factor is seen in clients with rheumatoid arthritis. A positive rheumatoid factor means that the antibody is detected in the blood. A positive rheumatoid factor is more likely to occur in clients with rheumatoid arthritis, especially during a flareup of the disease.
Choice D reason: Factor does not change is not seen in clients with rheumatoid arthritis. Rheumatoid factor can vary over time and may change depending on the activity of the disease. Rheumatoid factor may increase during a flareup and decrease during remission.
Correct Answer is ["A","B"]
Explanation
Choice A reason: Polyuria is the production of abnormally large amounts of urine, which can be caused by various factors, such as diabetes, kidney disease, or diuretics. Polyuria is not an expected finding in a client with inflammation, which is the body's response to injury or infection. Inflammation does not affect the urinary system directly, unless the inflammation is located in the kidneys or bladder.
Choice B reason: Edema is the swelling of tissues due to excess fluid accumulation, which can be caused by various factors, such as heart failure, liver disease, or venous insufficiency. Edema is not an expected finding in a client with inflammation, which is the body's response to injury or infection. Inflammation does not cause fluid retention, but rather fluid leakage from the blood vessels into the interstitial spaces.
Choice C reason: Heat is an expected finding in a client with inflammation, which is the body's response to injury or infection. Heat is caused by the increased blood flow to the inflamed area, which brings more oxygen and nutrients to the damaged tissues. Heat also helps to kill or inhibit the growth of microorganisms that may cause infection.
Choice D reason: Erythema is an expected finding in a client with inflammation, which is the body's response to injury or infection. Erythema is the redness of the skin due to the dilation of the blood vessels in the inflamed area, which increases the blood flow and the delivery of oxygen and nutrients to the damaged tissues. Erythema also helps to signal the presence of inflammation and attract immune cells to the site.
Choice E reason: Pain is an expected finding in a client with inflammation, which is the body's response to injury or infection. Pain is caused by the stimulation of the nerve endings by chemical mediators, such as histamine, prostaglandins, and bradykinin, that are released by the inflamed tissues. Pain also helps to alert the client of the injury or infection and to limit the movement or use of the affected area.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today