The nurse is caring for a 4-month-old infant in the emergency department. The nurse reviews the infant's medical record and assessment findings. Which of the following conditions should the nurse suspect, and what actions should the nurse take to address that condition, and what parameters should the nurse monitor to assess the infant's progress?
The nurse should suspect that the infant has
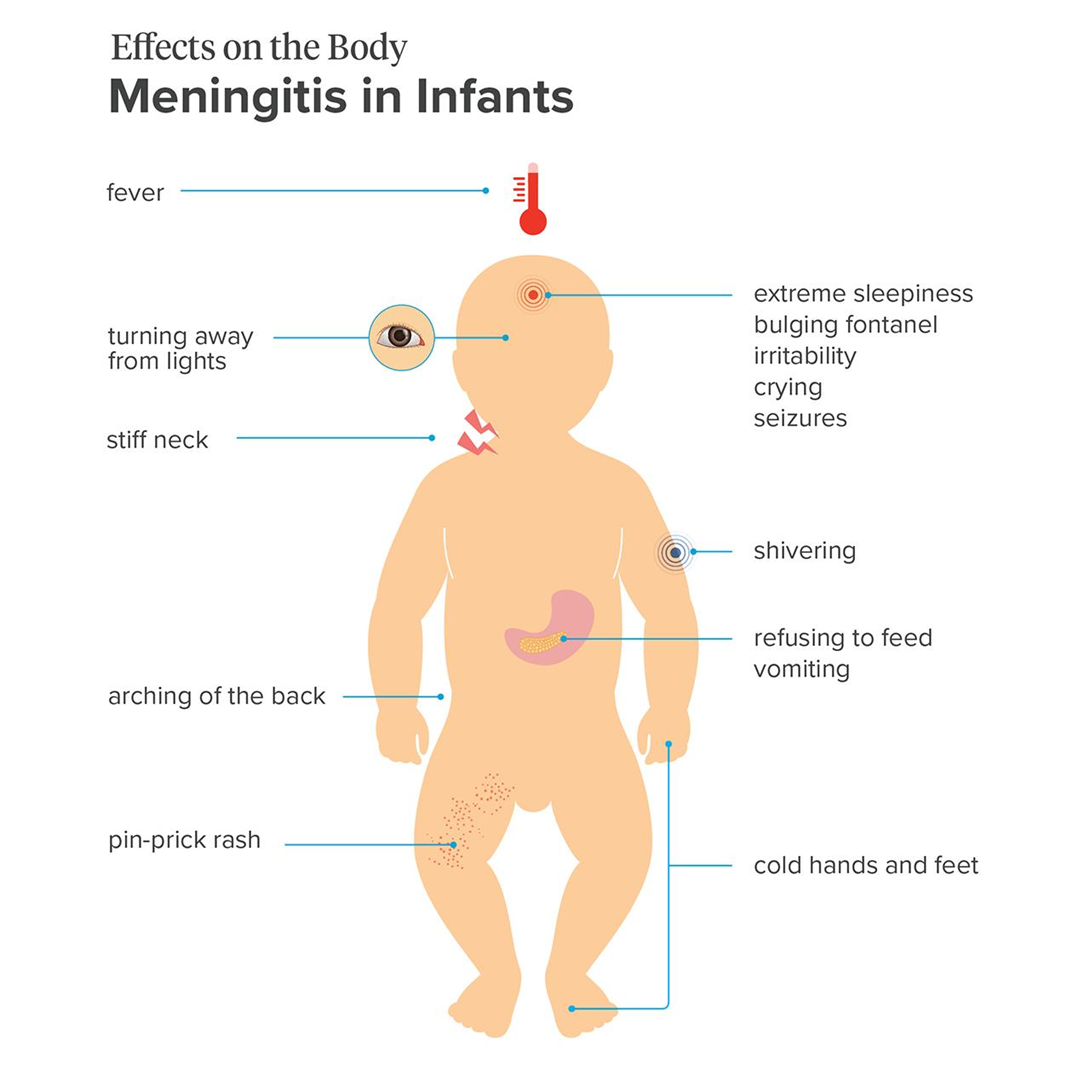
meningitis.
hydrocephalus.
intracranial hemorrhage.
sepsis.
The Correct Answer is A
Choice A reason: Meningitis is a possible condition, as it is an inflammation of the membranes that cover the brain and spinal cord. It can be caused by various microorganisms, such as bacteria, viruses, or fungi. The infant has many signs and symptoms of meningitis, such as fever, irritability, lethargy, bulging fontanel, and clear cerebrospinal fluid from the lumbar puncture.
Choice B reason: Hydrocephalus is not a likely condition, as it is an accumulation of cerebrospinal fluid in the brain, which causes increased intracranial pressure and enlargement of the head. The infant has a bulging fontanel, which can indicate increased intracranial pressure, but not necessarily hydrocephalus. The infant does not have other signs of hydrocephalus, such as a rapidly increasing head circumference, prominent scalp veins, or sunset eyes.
Choice C reason: Intracranial hemorrhage is not a probable condition, as it is a bleeding within the skull, which can result from trauma, vascular malformation, or coagulation disorder. The infant has retinal hemorrhages, which can indicate intracranial hemorrhage, but not necessarily. The infant does not have other signs of intracranial hemorrhage, such as seizures, vomiting, or altered mental status.
Choice D reason: Sepsis is not a definite condition, as it is a systemic inflammatory response to an infection, which can cause organ dysfunction and shock. The infant has a fever, which can indicate sepsis, but not necessarily. The infant does not have other signs of sepsis, such as tachycardia, tachypnea, hypotension, or poor perfusion.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: Maintaining the infant in the supine position is not an appropriate intervention, as it can increase the pressure on the myelomeningocele sac and cause further damage to the spinal cord. The nurse should position the infant prone or side-lying, with the head turned to one side and the hips flexed.
Choice B reason: Limiting visitors to immediate family members is not a necessary intervention, as the infant does not have an infectious condition that requires isolation. The nurse should encourage the parents and other family members to visit and bond with the infant, and provide emotional support and education.
Choice C reason: Initiating contact precautions is not a required intervention, as the infant does not have a contagious condition that poses a risk of transmission to others. The nurse should follow standard precautions, such as washing hands, wearing gloves, and disposing of contaminated materials properly.
Choice D reason: Providing a latex-free environment is an essential intervention, as the infant has a high risk of developing a latex allergy due to the frequent exposure to latex products during surgery and other procedures. The nurse should avoid using latex gloves, catheters, syringes, bandages, or other items that contain latex, and use alternative materials instead. The nurse should also label the infant's chart, crib, and door with a latex allergy alert.
Correct Answer is A
Explanation
Choice A reason: This is the correct instruction for the nurse to include in the plan. Mumps is a viral infection that causes inflammation of the salivary glands. It is transmitted by respiratory droplets from coughing, sneezing, or talking. The nurse should initiate droplet precautions, which include wearing a surgical mask, gloves, and gown, and keeping the child in a private room or with other children who have mumps.
Choice B reason: This is not the correct instruction for the nurse to include in the plan. Airborne precautions are used for infections that are transmitted by small particles that can remain suspended in the air for long periods of time, such as tuberculosis, chickenpox, or measles. Mumps is not an airborne infection, and the nurse does not need to wear a respirator or place the child in a negative pressure room.
Choice C reason: This is not the correct instruction for the nurse to include in the plan. Contact precautions are used for infections that are transmitted by direct or indirect contact with the infected person or their environment, such as scabies, impetigo, or MRSA. Mumps is not a contact infection, and the nurse does not need to wear gloves and gown for all interactions with the child or use disposable equipment.
Choice D reason: This is not the correct instruction for the nurse to include in the plan. Standard precautions are the minimum level of infection control that should be used for all patients, regardless of their diagnosis or presumed infection status. They include hand hygiene, use of personal protective equipment, safe injection practices, and environmental cleaning. However, they are not sufficient for preventing the transmission of mumps, and the nurse should use additional precautions.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today