The nurse identifies several nursing problems for a client with paraplegia who has been having fecal incontinence and diarrhea. The client's parent is the primary caregiver. In planning care, the nurse should determine which problem is the highest priority?
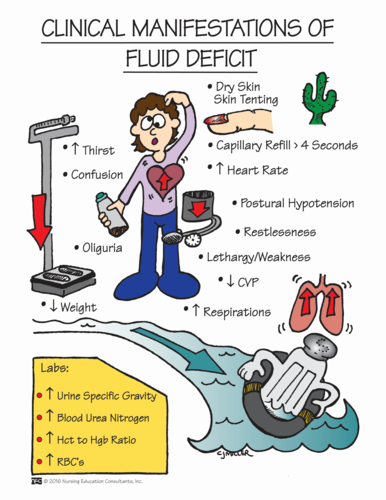
Fluid volume deficit.
Bowel incontinence.
Caregiver role strain.
Impaired bed mobility.
The Correct Answer is A
Choice A Reason: This is correct because fluid volume deficit is a life-threatening condition that can result from diarrhea and fecal incontinence. The nurse should monitor the client's fluid intake and output, electrolytes, weight, urine specific gravity, and skin turgor.
Choice B Reason: This is incorrect because bowel incontinence is a significant problem that can affect the client's dignity, comfort, and skin integrity, but it is not as urgent as fluid volume deficit. The nurse should implement a bowel management program and provide appropriate hygiene and skin care.
Choice C Reason: This is incorrect because caregiver role strain is a potential problem that can affect the parent's well-being and ability to provide care, but it is not as critical as fluid volume deficit. The nurse should assess the parent's coping skills, support system, and respite needs.
Choice D Reason: This is incorrect because impaired bed mobility is a chronic problem that can affect the client's functional status and quality of life, but it is not as serious as fluid volume deficit. The nurse should assist the client with positioning, turning, transferring, and exercising.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: This is incorrect because positioning the head with the chin tilted slightly downward can help prevent aspiration by closing the airway and directing food to the back of the throat.
Choice B Reason: This is correct because 60degrees is not fully upright and may not provide optimal protection against aspiration. The client should ideally be positioned at 90 degrees during meals if tolerated indicating need for additional teaching
Choice C Reason: This is incorrect because placing food on the unaffected side of the mouth can help prevent aspiration by stimulating the intact nerves and muscles that control swallowing.
Choice D Reason: This is incorrect because resting before meals decreases fatigue and improves swallowing ability.
Correct Answer is C
Explanation
Choice A Reason: This is incorrect because contacting the healthcare provider about the frequency of pain medication is a dependent intervention that requires an order from the provider. The nurse should first use independent interventions such as reviewing available prescriptions or providing non-pharmacological measures.
Choice B Reason: This is incorrect because encouraging the client to allow more time for the medication to work can imply that the nurse does not believe or validate the client's report of pain. It also can delay effective pain relief and increase suffering.
Choice C Reason: This is correct because reviewing the medical record for additional pain medication prescriptions can help identify alternative or adjunctive options for pain management, such as breakthrough doses, rescue doses, or non-opioid analgesics.
Choice D Reason: This is incorrect because administering an additional dose of morphine sulfate 0.2 mg intravenously can cause overdose, respiratory depression, or addiction. The nurse should follow the prescribed dosage, route, and interval of administration and monitor for adverse effects.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today