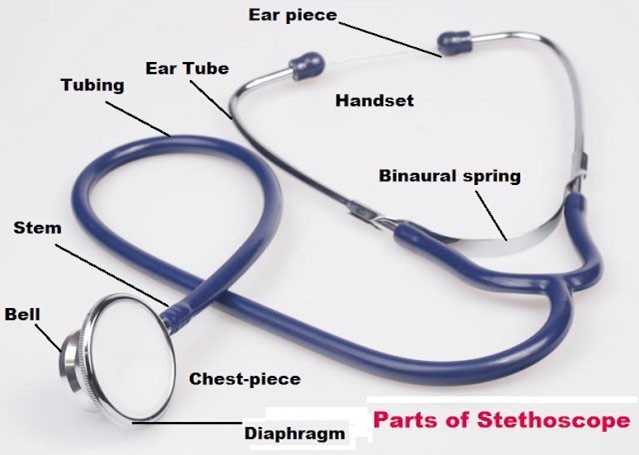
The nurse is assessing the lung sounds of a preschooler. Which action should the nurse implement to ensure the child's cooperation?
Have the child blow a cotton ball and have the parent catch it.
Place a toy in the child's hands while listening to the breath sounds.
Offer the child bubbles before the stethoscope is placed.
Allow the child to use a stethoscope on a stuffed animal.
The Correct Answer is D
To ensure the cooperation of a preschooler during an assessment of lung sounds, the nurse can allow the child to use a stethoscope on a stuffed animal. This helps the child understand what is happening and feel more comfortable with the procedure. Having the child blow a cotton ball (A), placing a toy in the child's hands (B), and offering bubbles (C ) may distract the child but do not directly involve them in the procedure.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Answer: (B) Counsel the client about the risks and benefits of using oral contraceptives.
Rationale:
(A) Encourage the client to discuss her need for contraceptives with her parents: Encouraging open communication with parents is important, but this action might not be the most appropriate in this context. The client has expressed a desire for confidentiality, and respecting her autonomy is essential, particularly when it comes to sensitive topics like sexual health.
(B) Counsel the client about the risks and benefits of using oral contraceptives: Providing counseling about the risks and benefits of oral contraceptives is the most appropriate action. It ensures the client is informed and able to make a decision that is right for her health and circumstances. The nurse can also discuss other contraceptive options and provide education on safe sex practices. This approach respects the client's autonomy and privacy while ensuring she receives the necessary information to make an informed choice.
(C) Explain that she needs parental approval to receive contraceptives: In many areas, adolescents have the right to obtain contraceptives without parental consent. Requiring parental approval might not only be legally incorrect but could also discourage the client from seeking necessary healthcare, potentially putting her at risk.
(D) Tell the client how to receive a variety of free oral contraceptives from the clinic: While providing information about accessing contraceptives is helpful, this option alone does not address the need for thorough counseling about the risks and benefits. It's important to ensure that the client understands the implications of using oral contraceptives and has the opportunity to ask questions and receive guidance tailored to her individual needs.
Correct Answer is C
Explanation
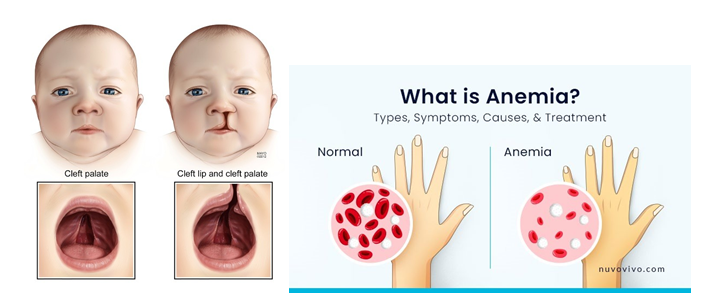
Answer: C. Red blood cell count of 2.3 cells/mcl or (2.3 x 10/L).
Rationale:
A. White blood cell count of 10,000/mm³ (10 x 10⁹/L): This is within the normal range for an infant, indicating no immediate concern for infection or immune response. It does not need to be urgently conveyed to the surgeon.
B. Weight gain of 2 pounds (0.91 kg) since birth: This is a positive sign indicating healthy growth and nutritional status, but it is not a critical concern that would affect the immediate surgical plan.
C. Red blood cell count of 2.3 cells/mcl or (2.3 x 10⁹/L): This low RBC count indicates anemia, which is critical information for the surgeon. Anemia can increase the risk of complications during and after surgery due to potential issues with oxygenation and healing, making it the most important information to convey.
D. Urine specific gravity is 1.011: This indicates normal hydration status and is not immediately relevant to the surgical procedure. It does not need to be urgently reported to the surgeon compared to the low RBC count.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today