The nurse leading a care team on a medical surgical unit is assigning client care to a practical nurse (PN) and an unlicensed assistive personnel (UAP). Which task should the nurse delegate to the PN?
Begin initial sterile wound care for surgical clients.
Validate prescribed intravenous flow rates.
Determine the need for urinary catheterizations.
Receive a postoperative client and conduct the assessment.
The Correct Answer is B
Choice A Reason: Beginning initial sterile wound care for surgical clients is a nursing intervention that requires clinical judgment and cannot be delegated to the PN. The PN may assist with wound care after the initial dressing change, but the RN is responsible for assessing the wound and initiating the plan of care.
Choice B Reason: Validating prescribed intravenous flow rates is a routine task that does not require clinical judgment and can be delegated to the PN. The PN has the knowledge and skill to check the IV orders, calculate the drip rate, and monitor the infusion.
Choice C Reason: Determining the need for urinary catheterizations is a nursing assessment that requires clinical judgment and cannot be delegated to the PN. The PN may perform urinary catheterizations as ordered by the physician, but the RN is responsible for evaluating the indication, risk, and benefit of the procedure.
Choice D Reason: Receiving a postoperative client and conducting the assessment is a nursing intervention that requires clinical judgment and cannot be delegated to the PN. The RN is responsible for receiving reports from the operating room, assessing the client's status, identifying potential complications, and initiating the plan of care.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: A subtotal thyroidectomy is a major surgery that involves the removal of part of the thyroid gland. The client may have complications such as bleeding, infection, hypocalcemia, or vocal cord damage. The client also needs close monitoring of vital signs, blood transfusion, and airway patency. This client is not stable enough to be transferred to a general unit.
Choice B Reason: A combined partial and full-thickness burn is a serious injury that involves damage to the epidermis, dermis, and underlying tissues. The client may have complications such as infection, fluid loss, hypovolemia, shock, or respiratory distress. The client also needs wound care, pain management, fluid replacement, and oxygen therapy. This client is not stable enough to be transferred to a general unit.
Choice C Reason: A renal transplant is a major surgery that involves the replacement of a diseased kidney with a healthy one from a donor. The client may have complications such as rejection, infection, bleeding, thrombosis, or urinary obstruction. The client also needs immunosuppressive therapy, anti-infective therapy, fluid and electrolyte balance, and pain management. This client is not stable enough to be transferred to a general unit.
Choice D Reason: Nephrotic syndrome is a kidney disorder that causes excessive protein loss in the urine, leading to low serum protein levels and edema. The client may have complications such as infection, thromboembolism, or malnutrition. The client needs diuretic therapy, protein replacement, dietary modification, and infection prevention. This client is relatively stable and can be transferred to a general unit.
Correct Answer is A
Explanation
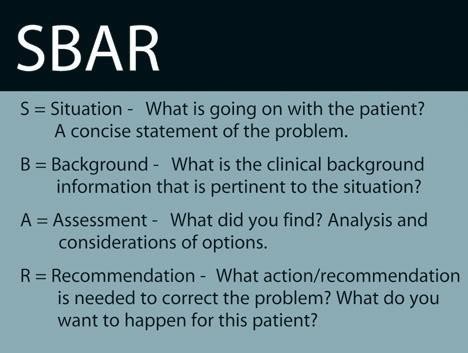
Choice A Reason: This is the best action because it describes the current situation of the client and alerts the family to a possible change in the client's status. The nurse should provide the most relevant and urgent information first using the SBAR communication.
Choice B Reason: This is not the first action because it does not address the current situation of the client. The nurse should verify the client's healthcare power of attorney, but this is not a priority at this time.
Choice C Reason: This is not the first action because it does not explain the cause of the client's confusion. The nurse should review the client's medications and assess for any adverse effects, but this is not a priority at this time.
Choice D Reason: This is not the first action because it provides background information that is not directly related to the current situation of the client. The nurse should give a brief history of the client's admission, but this can be done later.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today