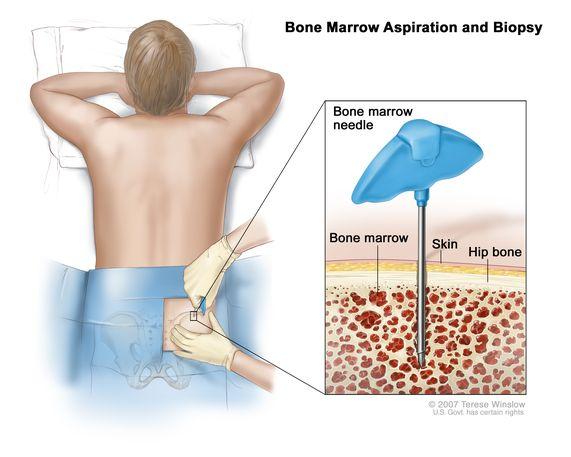
The nurse understands that a client who has had a bone marrow aspiration to assist in the diagnosis of aplastic anemia requires additional teaching when they state:
I can have aspirin 650 mg for pain when the procedure is over.
The nurse will check the puncture site at least every 4 hours after the procedure.
I will have some pain that is similar to a toothache.
I understand that this is a sterile procedure.
The Correct Answer is A
Choice A reason: The client requires additional teaching if they state that they can have aspirin for pain after the bone marrow aspiration. Aspirin is a drug that inhibits platelet aggregation and increases the risk of bleeding. ¹ The client should avoid aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) for at least 48 hours after the procedure. ² The client should use acetaminophen or another pain reliever that does not affect blood clotting.
Choice B reason: The client does not require additional teaching if they state that the nurse will check the puncture site at least every 4 hours after the procedure. This is a correct statement, as the nurse should monitor the site for signs of bleeding, infection, or hematoma. ² The nurse should also apply pressure and a sterile dressing to the site and instruct the client to keep it dry and clean for 24 hours.
Choice C reason: The client does not require additional teaching if they state that they will have some pain that is similar to a toothache. This is a correct statement, as the client may experience mild to moderate pain at the site of the aspiration, which may radiate to the hip or back. ² The pain usually subsides within a few hours or days.
Choice D reason: The client does not require additional teaching if they state that they understand that this is a sterile procedure. This is a correct statement, as the bone marrow aspiration is performed under sterile conditions to prevent infection. ² The nurse should wear gloves, gown, mask, and eye protection and use a sterile needle, syringe, and antiseptic solution.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: I will call dietary to bring you breakfast is not the best response by the nurse. This response may imply that the nurse is willing to compromise the test results or the client's safety by allowing them to eat before the test. The nurse should explain the rationale for fasting and offer the client some water or ice chips if allowed.
Choice B reason: Food may interact with the dye that is used for the test is not the best response by the nurse. This response may be partially true, but it is not specific or clear enough to justify the need for fasting. The nurse should explain that food can affect the absorption and distribution of the radioactive tracer that is injected into the bloodstream for the test, and that eating can also interfere with the quality of the images.
Choice C reason: I will ask the health care provider if the test can be rescheduled is not the best response by the nurse. This response may suggest that the nurse is not confident or knowledgeable about the test protocol or the client's condition. The nurse should explain the importance and urgency of the test and reassure the client that they will be able to eat after the test is done.
Choice D reason: The procedure is usually completed on an empty stomach is the best response by the nurse. This response is accurate and concise, and it informs the client of the standard preparation for the test. The nurse should also provide more details about the test procedure and the expected duration, and answer any questions or concerns that the client may have.
Correct Answer is C
Explanation
Choice A reason: Having a urinary output of greater than 30 mL per hour for 24 hours is not the most appropriate outcome for the problem of impaired tissue perfusion. This outcome is more relevant for the problem of fluid volume excess or renal impairment, which are not the case for this client.
Choice B reason: Discussing which lifestyle modifications will be necessary to maintain health is not the most appropriate outcome for the problem of impaired tissue perfusion. This outcome is more relevant for the problem of knowledge deficit or risk for recurrence, which are not the priority for this client.
Choice C reason: Expressing no complaints of chest discomfort or shortness of breath is the most appropriate outcome for the problem of impaired tissue perfusion. This outcome indicates that the client's cardiac output and oxygen delivery are adequate and that the interventions are effective.
Choice D reason: Having clear breath sounds bilaterally upon auscultation is not the most appropriate outcome for the problem of impaired tissue perfusion. This outcome is more relevant for the problem of impaired gas exchange or pulmonary congestion, which are not the case for this client.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today