The parents of a newborn who is being treated for bacterial septicemia ask the nurse why their baby didn't seem very ill. The best response of the nurse is:
Select one:
"You would have seen more symptoms if you had been looking more closely at your baby."
"A newborn's immune system isn't mature, so symptoms are subtle and can be hard to recognize."
"A high fever will always be present in sick newborns, including your baby."
"A mother's immunity usually protects the infant from illness, but not in this case."
The Correct Answer is B
Choice A Reason: "You would have seen more symptoms if you had been looking more closely at your baby." This is an inappropriate response that blames the parents for missing the signs of sepsis and does not explain the Reason for the subtle symptoms.
Choice B Reason: "A newborn's immune system isn't mature, so symptoms are subtle and can be hard to recognize." This is an appropriate response that educates the parents about the immunological basis of sepsis in newborns and reassures them that they are not at fault for not noticing the symptoms.
Choice C Reason: "A high fever will always be present in sick newborns, including your baby." This is an incorrect response that contradicts the fact that newborns may not develop fever in response to infection due to their immature immune systems.
Choice D Reason: "A mother's immunity usually protects the infant from illness, but not in this case." This is an inaccurate response that implies that the mother failed to provide adequate immunity to her baby and does not address the question of why the baby did not seem very ill.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
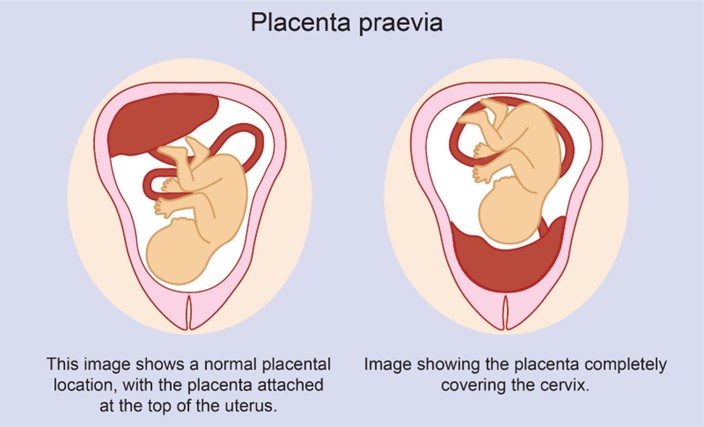
Choice A Reason: Partial placenta previa is a condition where the placenta partially covers the cervix. It usually does not resolve and may cause bleeding and complications during labor and delivery.
Choice B Reason: Complete placenta previa is a condition where the placenta completely covers the cervix. It is a serious condition that requires cesarean delivery and may cause life-threatening hemorrhage.
Choice C Reason: Marginal placenta previa is a condition where the edge of the placenta reaches the margin of the cervix. It may also cause bleeding and complications during labor and delivery.
Choice D Reason: Low-lying placenta previa is a condition where the placenta is near the cervix, but not covering it. It may resolve spontaneously as the uterus grows and the placenta moves upward.
Correct Answer is A
Explanation
Choice A Reason: Insulin needs decrease in the first trimester, but increase in the second trimester as the woman's body becomes more insulin-resistant. This is because this statement describes the typical patern of insulin requirements during pregnancy for women with pre-existing diabetes. Insulin needs decrease in the first trimester due to increased insulin production by the pancreas, increased insulin sensitivity by the tissues, and increased risk of hypoglycemia due to nausea and vomiting. Insulin needs increase in the second trimester due to increased levels of placental hormones such as human placental lactogen (hPL), which antagonize insulin action and cause insulin resistance.
Choice B Reason: Vascular disease that always accompanies diabetes slows fetal growth. This is an incorrect answer that makes a false and exaggerated claim about diabetes and fetal growth. Vascular disease does not always accompany diabetes, but it can be a complication of long-term or poorly controlled diabetes that affects blood vessels and circulation. Vascular disease can affect fetal growth by reducing placental perfusion and oxygen delivery, but it is not the only factor that influences fetal growth. Other factors include maternal nutrition, genetics, infections, or anomalies.
Choice C Reason: The risk of ketoacidosis decreases during the length of the pregnancy. This is an incorrect answer that contradicts the evidence and guidelines on diabetes and ketoacidosis during pregnancy. Ketoacidosis is a metabolic emergency where high levels of ketones accumulate in the blood due to insufficient insulin or excessive glucose utilization, which causes acidosis, dehydration, electrolyte imbalance, and coma. Ketoacidosis can occur in women with diabetes during pregnancy due to infection, stress, starvation, or inadequate insulin therapy. The risk of ketoacidosis does not decrease during the length of the pregnancy, but rather increases in the second and third trimesters due to increased insulin resistance and glucose production.
Choice D Reason: The baby is likely to have a congenital abnormality because of the uncontrolled diabetes. This is an incorrect answer that implies a negative and deterministic outcome for the baby. Congenital abnormalities are structural or functional defects that are present at birth, which can affect various organs or systems in the baby.
Congenital abnormalities can be caused by genetic or environmental factors, or a combination of both. Diabetes can increase the risk of congenital abnormalities, especially if the blood glucose levels are high during the first trimester, when organogenesis occurs. However, the risk of congenital abnormalities is not inevitable or predictable, and it can be reduced by maintaining good glycemic control before and during pregnancy.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today