The practical nurse (PN) determines that a client's pupils constrict as they change focus from a far object to a near object. How should the PN document this finding?
Peripheral vision intact.
Nystagmus present with pupillary focus.
Consensual pupillary constriction present
Pupils reactive to accommodation
The Correct Answer is D
The correct answer is choice D, Pupils reactive to accommodation. Choice A rationale:
"Peripheral vision intact”. refers to the ability to see objects at the outer edges of one's visual field. It is not relevant to the assessment of pupillary response and does not describe the finding of pupils constricting as they change focus from a far object to a near object.
Choice B rationale:
"Nystagmus present with pupillary focus”. suggests involuntary rapid eye movements accompanied by changes in pupillary response. Nystagmus is not an expected finding during pupillary accommodation, and its presence would indicate a neurological issue rather than a normal response.
Choice C rationale:
"Consensual pupillary constriction present”. refers to both pupils constricting when light is shined into one eye. While this finding is normal, it does not specifically describe the pupils' response during accommodation when focusing from a far object to a near object.
Choice D rationale:
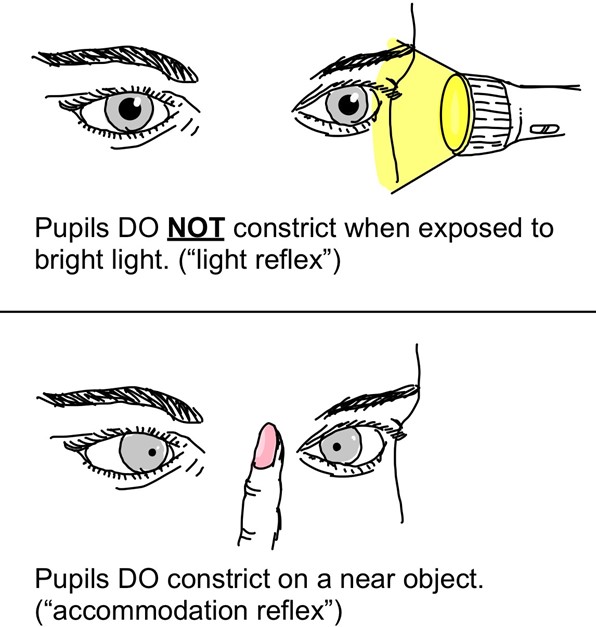
"Pupils reactive to accommodation”. accurately describes the normal physiological response of the pupils constricting as they change focus from a distant object to a nearby object. This response ensures that the appropriate amount of light enters the eyes to maintain clear vision during different distances of focus.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
This is the best action for the PN to use in assisting this client to deal with his pain because it provides a non-pharmacological method of pain relief that can enhance the effect of the opioid analgesic. Slow, rhythmic breathing can help the client relax, distract from the pain, and increase oxygenation and blood flow.
A. Dimming the lights in the room and closing the door may not be enough to help the client deal with his pain and may not address his psychological or emotional needs.
C. Turning the television on to the client's favorite show may not be effective in helping the client deal with his pain and may be distracting or irritating for him.
D. Obtaining a prescription for a higher dose of pain medication may not be necessary or appropriate for this client and may increase the risk of side effects or dependence. The PN should assess the client's pain level and response to the current dose before requesting a change in medication.
Correct Answer is B
Explanation
The correct answer is choice B. Attach the drainage bag to the bed frame.
Choice A rationale:
Measuring the urinary output in the bag is a routine task but does not address the improper placement of the drainage bag. The immediate concern is to ensure the drainage bag is correctly positioned to prevent complications.
Choice B rationale:
Attaching the drainage bag to the bed frame is the correct action. The drainage bag should be kept below the level of the bladder and attached to a non-movable part of the bed to prevent backflow and reduce the risk of infection.
Choice C rationale:
Applying gloves and emptying the drainage bag is not the immediate priority. The drainage bag should not be allowed to overfill, but in this scenario, it is only half-full, so this action is not urgent.
Choice D rationale:
Removing the looped tubing from the bed is important to ensure proper drainage and prevent backflow, but it does not address the incorrect placement of the drainage bag, which is the primary concern in this situation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today