When preparing to administer a prescribed medication to a homeless male at a community psychiatric clinic, the client tells the nurse that he usually takes a different dosage. Which action should the nurse take?
Explain to the client that the dosage has been changed.
Withhold the medication until the dosage can be confirmed.
Inform him that he may refuse the medication and document whether or not he takes it.
Tell him to take the medication then verify the dosage at the next healthcare team meeting.
The Correct Answer is B
Choice A reason: Explaining to the client that the dosage has been changed is not a safe action because it may not be true. The nurse should not assume that the prescribed dosage is correct or different from the previous one without verifying it with the healthcare provider or the medication record.
Choice B reason: This is the correct answer because withholding the medication until the dosage can be confirmed is a prudent action that ensures patient safety and avoids medication errors. The nurse should compare the prescribed dosage with the client's previous dosage and consult with the healthcare provider or the pharmacist if there is any discrepancy or doubt.
Choice C reason: Informing him that he may refuse the medication and documenting whether or not he takes it is not a responsible action because it does not address the issue of dosage discrepancy. The nurse should respect the client's right to refuse medication, but should also educate him about the benefits and risks of taking or not taking it. The nurse should also try to resolve any barriers or concerns that may affect the client's adherence to medication.
Choice D reason: Telling him to take the medication then verifying the dosage at the next healthcare team meeting is not a timely action because it may cause harm or complications to the client. The nurse should not administer any medication without checking its accuracy and appropriateness for the client. The nurse should also report and document any medication incidents as soon as possible.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: Measuring abdominal girth is not a specific assessment for a client with a suprapubic catheter, which is a tube inserted through the lower abdomen into the bladder to drain urine. However, it may be useful for monitoring fluid status and abdominal distension.
Choice B reason: Assessing perineal area is not a specific assessment for a client with a suprapubic catheter, which is a tube inserted through the lower abdomen into the bladder to drain urine. However, it may be important for maintaining hygiene and preventing infection.
Choice C reason: This is the correct answer because observing insertionsite is a specific assessment for a client with a suprapubic catheter, which is a tube inserted through the lower abdomen into the bladder to drain urine. The nurse should inspect the incision site for signs of healing, infection, or leakage.
Choice D reason: Palpating flank area is not a specific assessment for a client with a suprapubic catheter, which is a tube inserted through the lower abdomen into the bladder to drain urine. However, it may be helpful for detecting kidney tenderness or enlargement.
Correct Answer is A
Explanation
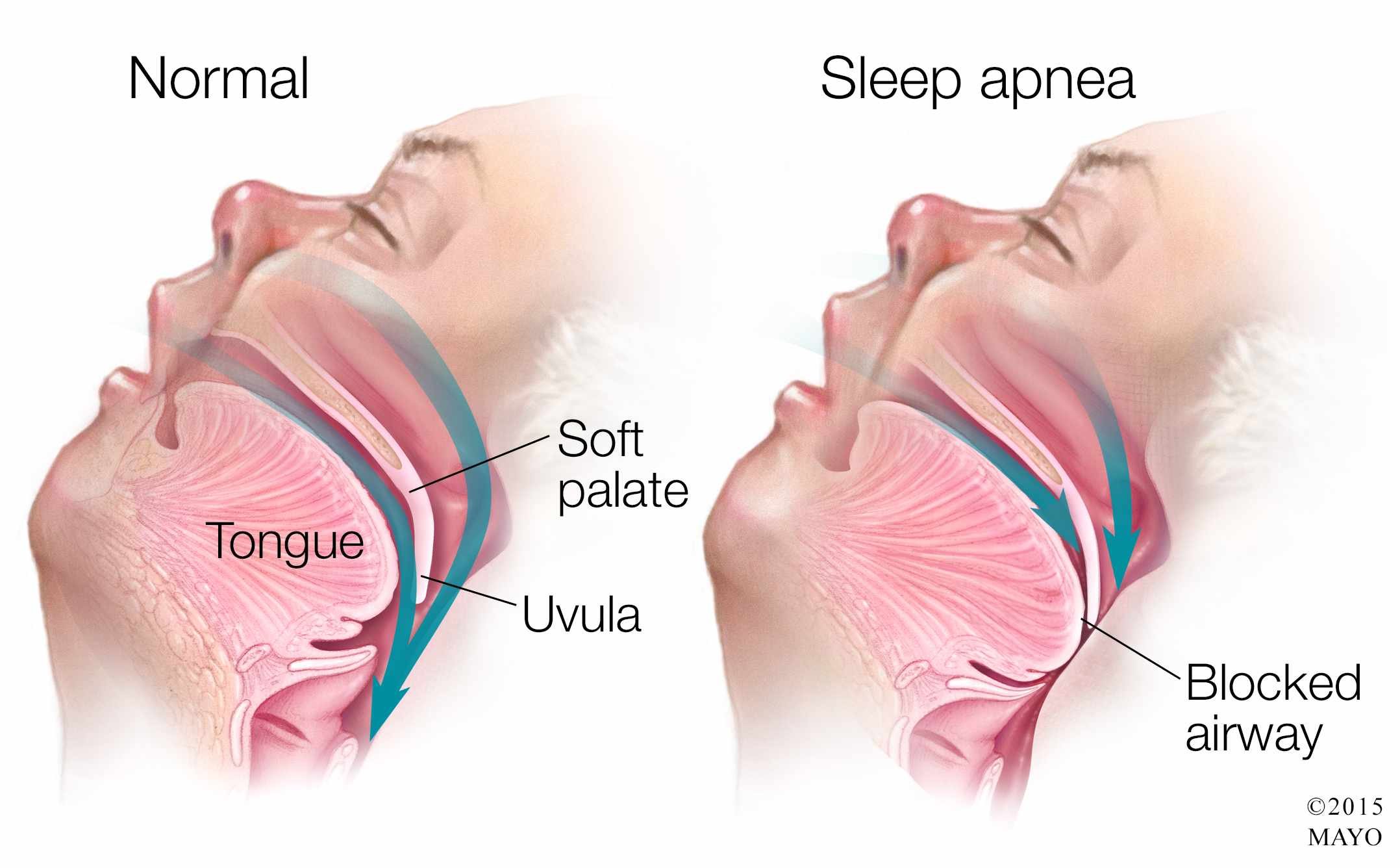
Choice A reason: This is the correct answer because applying the client's positive airway pressure device is the most important intervention for the nurse to implement before leaving the client. Positive airway pressure device is a treatment that delivers pressurized air through a mask or nasal prongs to keep the upper airway open and prevent apnea episodes during sleep. Obstructive sleep apnea is a condition that causes repeated interruptions in breathing due to partial or complete collapse of the upper airway during sleep. The nurse should ensure that the device is fitted properly and functioning well.
Choice B reason: Elevating the head of the bed to a 45 degree angle is not a sufficient intervention for the nurse to implement before leaving the client. Elevating the head of the bed can help reduce snoring and improve breathing by preventing the tongue and soft palate from falling back and obstructing the airway. However, it may not be enough to prevent apnea episodes in clients with obstructive sleep apnea, especially if they have other risk factors such as obesity, enlarged tonsils, or nasal congestion. The nurse should also use other interventions such as positive airway pressure device, weight loss, or surgery.
Choice C reason: Removing dentures or other oral appliances is not a relevant intervention for the nurse to implement before leaving the client. Dentures or other oral appliances are devices that replace missing teeth or improve dental alignment. They may help improve speech, chewing, and appearance, but they do not have a direct impact on obstructive sleep apnea. The nurse should instruct the client to remove dentures or other oral appliances before going to bed to prevent discomfort, infection, or damage.
Choice D reason: Lifting and locking the side rails in place is not a necessary intervention for the nurse to implement before leaving the client. Side rails are bars that attach to the sides of the bed frame to prevent falls or injuries. They may provide safety and security for some clients, but they may also pose risks such as entrapment, strangulation, or agitation. The nurse should assess the need for side rails on an individual basis and consider alternative measures such as bed alarms, low beds, or floor mats.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today