Which action is essential when assessing for drainage in a client with a large abdominal wound?
Feel the top of the client’s legs.
Examine area underneath the client.
Ask the client to cough forcefully.
Have the client sit up and lean forward.
The Correct Answer is B
This is essential because drainage from a large abdominal wound may collect under the client and be missed if only the dressing is inspected. The amount, color, and consistency of drainage should be documented and reported to the health care provider.
Choice A is wrong because feeling the top of the client’s legs will not help assess for drainage in a large abdominal wound.
Choice C is wrong because asking the client to cough forcefully may increase the risk of dehiscence (separation of wound edges) or evisceration (protrusion of internal organs through the wound) in a large abdominal wound.
Choice D is wrong because having the client sit up and lean forward may also increase the risk of dehiscence or evisceration in a large abdominal wound.
Normal ranges for wound drainage depend on the type, location, and size of the wound, as well as the stage of healing. Generally, drainage should decrease over time and change from bloody to serous.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
This is because it shows a normal pH, pCO2, HCO3 and pO2, indicating that the treatment has been effective in restoring normal gas exchange and acid- base balance.
Choice A is wrong because it shows a low pH, high pCO2 and high HCO3, indicating a mixed respiratory and metabolic acidosis.
Choice B is wrong because it shows a low pH, high pCO2 and low HCO3, indicating a combined respiratory and metabolic acidosis.
Choice D is wrong because it shows a high pH, low pCO2 and low HCO3, indicating a mixed respiratory and metabolic alkalosis.
The normal ranges for arterial blood gas (ABG) are:
- pH: 7.35 – 7.45
- pO2: 10 – 14 kPa or 75 – 105 mmHg
- pCO2: 4.5 – 6 kPa or 34 – 45 mmHg
Correct Answer is B
Explanation
This is because non-steroidal anti-inflammatory drugs (NSAIDs) are medicines that are used to treat rheumatoid arthritis by reducing pain, inflammation, and swelling.
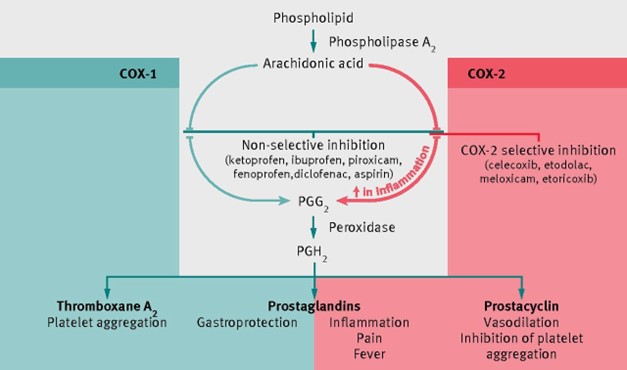
However, NSAIDs do not slow down the disease progression or prevent joint
damage. Therefore, they are often used along with other types of medications, such as methotrexate or biologics, that can modify the disease course. NSAIDs may take up to two weeks to reach their full anti-inflammatory effect.
Choice A is wrong because using aspirin to relieve other types of pain can increase the risk of bleeding and stomach ulcers when taken with NSAIDs.
Choice C is wrong because taking the medication on an empty stomach can increase the risk of stomach irritation and ulcers.
Choice D is wrong because taking the medication after exercising does not prevent the progression of disease or joint damage.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today