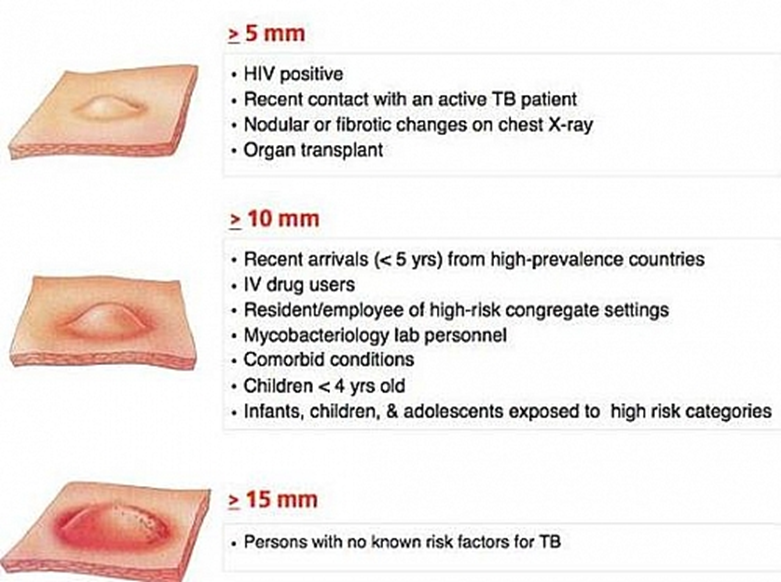
Which nursing assessment indicates a positive reading of a tuberculin (TB) skin test?
1 day after injection with a 10-mm area of redness and swelling
2 days after injection with a 5-mm area of redness and swelling
4 days after injection with a 3-mm area of redness and swelling
5 days after injection with a 2-mm area of redness and swelling
The Correct Answer is A
A. 1 day after injection with a 10-mm area of redness and swelling:
This may suggest a positive reading, but induration size is the primary criterion for interpretation, not just redness and swelling.
B. 2 days after injection with a 5-mm area of redness and swelling:
Similar to option A, a 5-mm area of redness and swelling alone does not definitively indicate a positive TB skin test. Again, without information on the size of the induration, we cannot determine if this reading is positive.
C. 4 days after injection with a 3-mm area of redness and swelling:
Once more, a 3-mm area of redness and swelling alone does not definitively indicate a positive TB skin test. As with the previous options, the size of the induration is the critical factor for interpretation.
D. 5 days after injection with a 2-mm area of redness and swelling:
As with the other options, a 2-mm area of redness and swelling alone does not definitively indicate a positive TB skin test. The presence and size of induration are essential for accurate interpretation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. The spacer increases the amount of medication delivered to the oropharynx.
Spacers are designed to minimize the amount of medication deposited in the oropharynx (back of the throat) and reduce the risk of side effects such as oral thrush or hoarseness. The main purpose of using a spacer is to optimize the delivery of medication to the lungs.
B. The spacer increases the amount of medication delivered to the lungs.
When reinforcing teaching with the parents of a child who is starting to use a spacer with a metered-dose inhaler (MDI) to treat asthma, the nurse should include the information that the spacer increases the amount of medication delivered to the lungs. Spacers help improve the delivery of medication from the MDI to the lungs by reducing the need for coordination between actuation of the MDI and inhalation. They also slow down the speed of the aerosolized medication particles, allowing more time for them to be inhaled into the lungs effectively.
C. Inhale rapidly when using the spacer with the MDI.
Inhaling rapidly may lead to improper inhalation technique and reduce the effectiveness of medication delivery to the lungs. Instead, the child should be instructed to inhale slowly and deeply to ensure that the medication reaches the lower airways.
D. Cover exhalation slots of the spacer with lips when inhaling.
Covering the exhalation slots of the spacer with lips during inhalation is not recommended. These slots are designed to allow the child to exhale freely and prevent buildup of pressure within the spacer. Encouraging the child to exhale into the spacer would hinder proper inhalation technique and could lead to decreased medication delivery to the lungs.
Correct Answer is C
Explanation
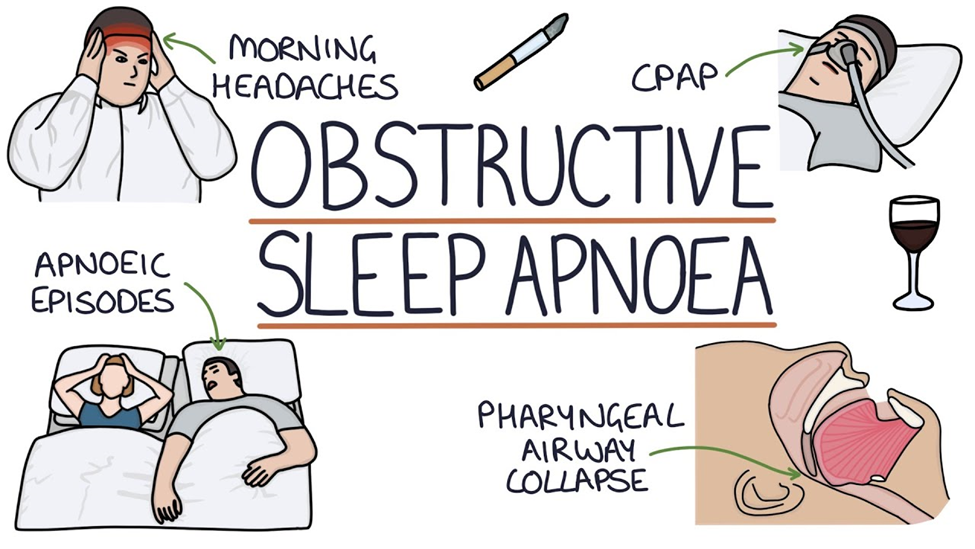
A. Constipation
Constipation is not typically associated with obstructive sleep apnea. However, sleep disturbances and certain medications used to manage OSA may indirectly contribute to constipation in some cases.
B. Nausea
Nausea is not a common symptom of obstructive sleep apnea. While sleep disturbances may affect gastrointestinal function in some individuals, nausea is not a typical manifestation of OSA.
C. Headache
One of the common findings associated with obstructive sleep apnea (OSA) is headache. This occurs due to the repeated episodes of apnea (cessation of breathing) during sleep, which leads to intermittent hypoxia (low oxygen levels) and subsequent cerebral vasodilation. The vasodilation can trigger headaches, often described as morning headaches, upon waking up. These headaches are typically frontal and may be accompanied by other symptoms such as fatigue and irritability.
D. Hypotension
Hypotension (low blood pressure) is not a typical finding in obstructive sleep apnea. In fact, individuals with OSA are more likely to have hypertension (high blood pressure) due to the effects of repeated apnea episodes on the cardiovascular system, such as increased sympathetic activity and arterial stiffness.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today