Which physiological change should a nurse expect to observe when assessing an elderly client?
Diminished attention span.
Decreased sensory acuity.
Increased need for rest.
Enhanced intestinal motility.
The Correct Answer is B
Decreased sensory acuity. This is a physiological change that occurs in elderly people due to the reduced function of the sensory organs, such as the eyes, ears, nose, tongue, and skin. Elderly people may experience impaired vision, hearing loss, reduced smell and taste, and decreased touch sensitivity.
Choice A is wrong because diminished attention span is not a normal physiological change in elderly people. It may be a sign of cognitive impairment or dementia.
Choice C is wrong because the increased need for rest is not a normal physiological change in elderly people. It may be a sign of fatigue, depression, or medical conditions.
Choice D is wrong because enhanced intestinal motility is not a normal physiological change in elderly people. It may be a sign of gastrointestinal disorders or infections.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
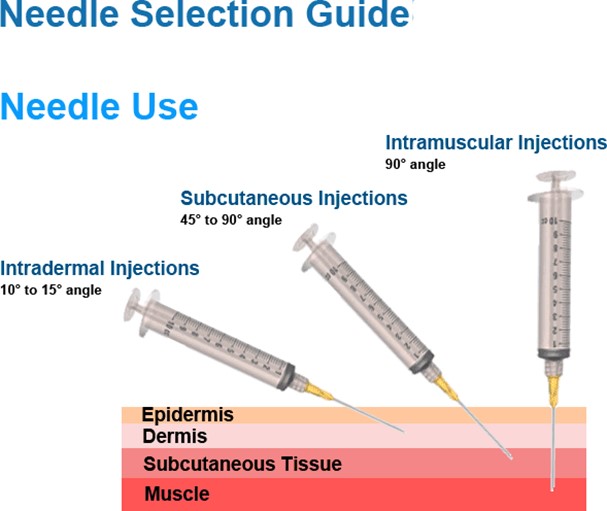
This needle size is appropriate for an intramuscular injection into the deltoid of a 175-pound adult male with a viscous fluid.
The needle length should be long enough to reach the muscle through the subcutaneous tissue, and the needle gauge should be suitable for the viscosity of the fluid. A 23-gauge needle is a common choice for intramuscular injections.
Choice A is wrong because a 1/2 inch needle is too short to reach the deltoid muscle in an adult male.
Choice C is wrong because a 1-1/2 inch needle is too long and may cause injury to the underlying nerves or blood vessels.
Choice D is wrong because a 16-gauge needle is too large and may cause excessive tissue trauma and pain.
Correct Answer is D
Explanation
The needle gauge size for subcutaneous injections should be between 25 and 31, depending on the patient’s size and the viscosity of the medication.
A smaller gauge number means a larger diameter needle, which can cause more pain and tissue damage.
Choice A is wrong because 8 is too large for subcutaneous injections and can cause bleeding and bruising.
Choice B is wrong because 20 is also too large for subcutaneous injections and can cause similar complications as choice A.
Choice C is wrong because 21 is still too large for subcutaneous injections and can cause discomfort and injury to the patient.
The needle length for subcutaneous injections should be between ½ inch and ⅝ inch, depending on the amount of subcutaneous tissue present. The nurse should pinch the skin and insert the needle at a 45-degree angle to ensure proper delivery of the medication.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today