
Ati Rn Custom Med Surg Surgical Patient Proctored Exam
Ati Rn Custom Med Surg Surgical Patient Proctored Exam
Total Questions : 53
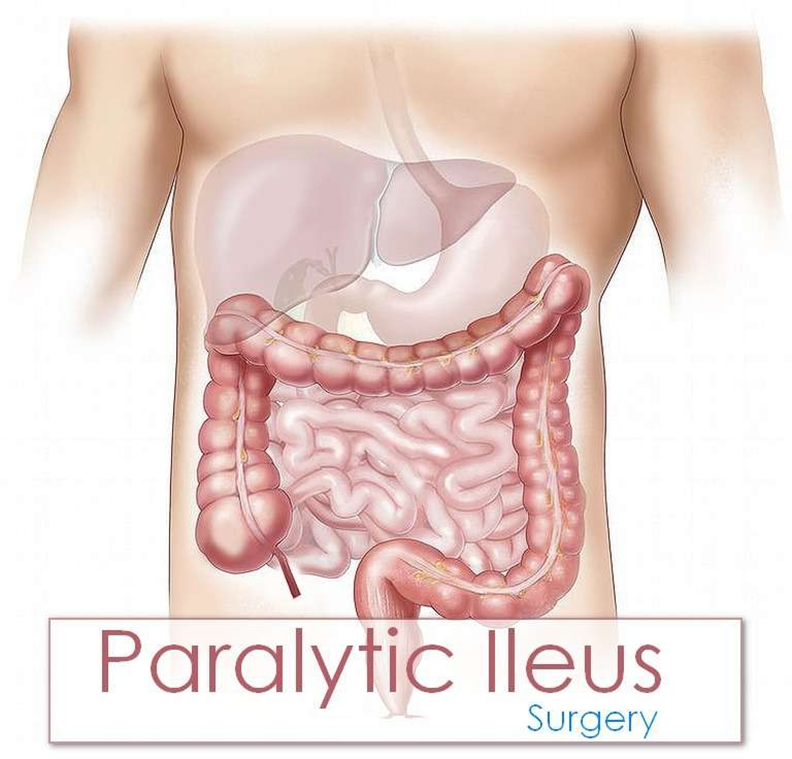
Showing 10 questions Sign up for moreA nurse is caring for a patient on the third day following abdominal surgery.
The nurse notes the absence of bowel sounds, abdominal distention, and the patient has not passed any flatus. Which postoperative complication is the patient likely experiencing?
Explanation
Choice A rationale:
Paralytic ileus is a common postoperative complication that occurs when the normal movement of the intestines (peristalsis) is slowed or stopped. This can lead to a buildup of gas and fluids in the intestines, causing abdominal distention, nausea, vomiting, and constipation. The absence of bowel sounds, abdominal distention, and the inability to pass flatus are all classic signs of paralytic ileus.
Here are some of the factors that can contribute to paralytic ileus: Manipulation of the intestines during surgery
Anesthesia
Pain medications, especially opioids Electrolyte imbalances
Dehydration
Underlying medical conditions, such as diabetes or kidney disease Treatment for paralytic ileus typically involves:
Resting the bowel by not eating or drinking anything by mouth
Using a nasogastric (NG) tube to suction out gas and fluids from the stomach Providing intravenous (IV) fluids and electrolytes
Encouraging early ambulation
Using medications to stimulate bowel movement, such as metoclopramide or erythromycin
Choice B rationale:
Incisional infection is an infection of the surgical wound. It would typically present with redness, warmth, swelling, and pain at the incision site. The patient may also have a fever. While incisional infections can occur after abdominal surgery, they are not typically associated with the absence of bowel sounds, abdominal distention, and the inability to pass flatus.
Choice C rationale:
Fecal impaction is a severe form of constipation in which a large, hard mass of stool becomes trapped in the rectum. It can cause abdominal pain, bloating, and difficulty passing stool. However, it is not typically associated with the absence of bowel sounds or abdominal distention.
Choice D rationale:
Health care-associated Clostridium difficile (C. difficile) is a bacterial infection that can cause severe diarrhea, abdominal pain, and cramping. It is often associated with antibiotic use. While C. difficile can occur after abdominal surgery, it is not typically associated with the absence of bowel sounds, abdominal distention, and the inability to pass flatus.
What should the nurse do in response to these inquiries?
Explanation
Rationale for Choice A:
Refer Questions to the Nursing Supervisor:
While it's essential to involve the nursing supervisor in situations that require their expertise or authority, it's not always necessary for basic inquiries about a patient's presence on the unit.
Disadvantages of referring calls to the nursing supervisor in this scenario:
It could delay the dissemination of essential information to concerned colleagues.
It could increase the workload of the nursing supervisor, potentially diverting their attention from more critical tasks. It could create a perception of a lack of transparency or openness among staff members.
Rationale for Choice B:
Transfer calls directly to the patient’s room:
Transferring calls directly to a patient's room without their consent breaches their privacy and confidentiality. It could also place undue stress on the patient, especially if they are not prepared to receive calls or discuss their health status.
Disadvantages of transferring calls directly to the patient’s room:
It violates the patient's right to privacy and confidentiality. It could disrupt the patient's rest and recovery.
It could place the patient in an uncomfortable position of having to answer questions about their health when they may not feel ready to do so.
Rationale for Choice C:
Acknowledge that the person is a patient on the unit, but give no specific details about the patient’s condition:
This approach strikes a balance between protecting the patient's privacy and providing necessary information to concerned colleagues. It verifies the patient's presence on the unit without disclosing any sensitive details about their health, thus adhering to ethical and legal guidelines.
Advantages of acknowledging the patient’s presence without providing details:
Respects the patient's right to privacy and confidentiality. Aligns with ethical and legal principles of healthcare.
Provides basic information to concerned colleagues without compromising patient information. Helps to establish trust and transparency among staff members.
Rationale for Choice D:
Contact the patient’s provider:
Contacting the patient's provider for every inquiry about the patient's presence is not practical or efficient. It could overburden the provider and delay the relay of information to concerned colleagues.
Explanation
Choice A rationale:
Notifying the facility's security department may be necessary in some cases, but it should not be the nurse's first action. This could escalate the situation and make the patient feel threatened or coerced. It's important to first attempt to de-escalate the situation and understand the patient's reasons for wanting to leave. Involving security prematurely could damage the nurse- patient relationship and make it more difficult to provide care in the future.
Security should be involved if the patient is a danger to themselves or others, or if they are attempting to leave in a way that could cause harm. However, in most cases, it is best to try to resolve the situation through communication and understanding.
Choice B rationale:
Calling the patient's family may be helpful in some cases, but it is not always necessary or appropriate. The nurse should first assess the patient's decision-making capacity and their understanding of the risks of leaving against medical advice. If the patient is capable of making their own decisions, the nurse should respect their autonomy and not involve family members without their consent.
Involving family members without the patient's consent could breach confidentiality and erode trust. It's important to balance the patient's right to privacy with the potential benefits of involving family members.
Choice C rationale:
Insisting that the patient exit the hospital via a wheelchair is not necessary in most cases. If the patient is able to walk and does not pose a safety risk, they should be allowed to leave on their own terms. Requiring a wheelchair could be seen as patronizing or controlling, and it could further upset the patient.
The use of a wheelchair should be based on the patient's individual needs and preferences, not on a blanket policy.
Choice D rationale:
Making sure the patient understands that they are leaving against medical advice is the most important action the nurse can take. This ensures that the patient is aware of the potential risks of leaving the hospital, and it protects the nurse from liability. The nurse should document the patient's decision in the medical record and have the patient sign an Against Medical Advice (AMA) form.
By ensuring informed consent, the nurse respects the patient's autonomy while also fulfilling their professional obligations.
Which patient should the nurse identify as having the highest risk for aspiration?
Explanation
Choice A rationale:
A colostomy is a surgical opening in the abdomen that allows stool to pass through the colon and out of the body. While a colostomy may increase the risk of certain complications, such as dehydration and skin irritation, it does not directly increase the risk of aspiration. This is because the colostomy bypasses the upper digestive tract, where aspiration typically occurs.
Choice B rationale:
An ileostomy is a similar surgical opening in the abdomen, but it diverts the small intestine rather than the colon. Like a colostomy, an ileostomy does not directly increase the risk of aspiration. However, it may lead to dehydration and electrolyte imbalances, which could indirectly contribute to aspiration risk.
Choice C rationale:
Enteral feedings through an NG tube are a common way to provide nutrition to patients who cannot eat by mouth. However, these feedings can also increase the risk of aspiration. This is because the NG tube bypasses the normal swallowing mechanisms, which help to protect the airway. If the feeding tube is not properly positioned or if the patient has impaired gastric motility, formula could enter the lungs and cause aspiration pneumonia.
Choice D rationale:
A chest tube is a drainage tube that is inserted into the chest cavity to remove air or fluid. While a chest tube may cause some discomfort and respiratory issues, it does not directly increase the risk of aspiration.
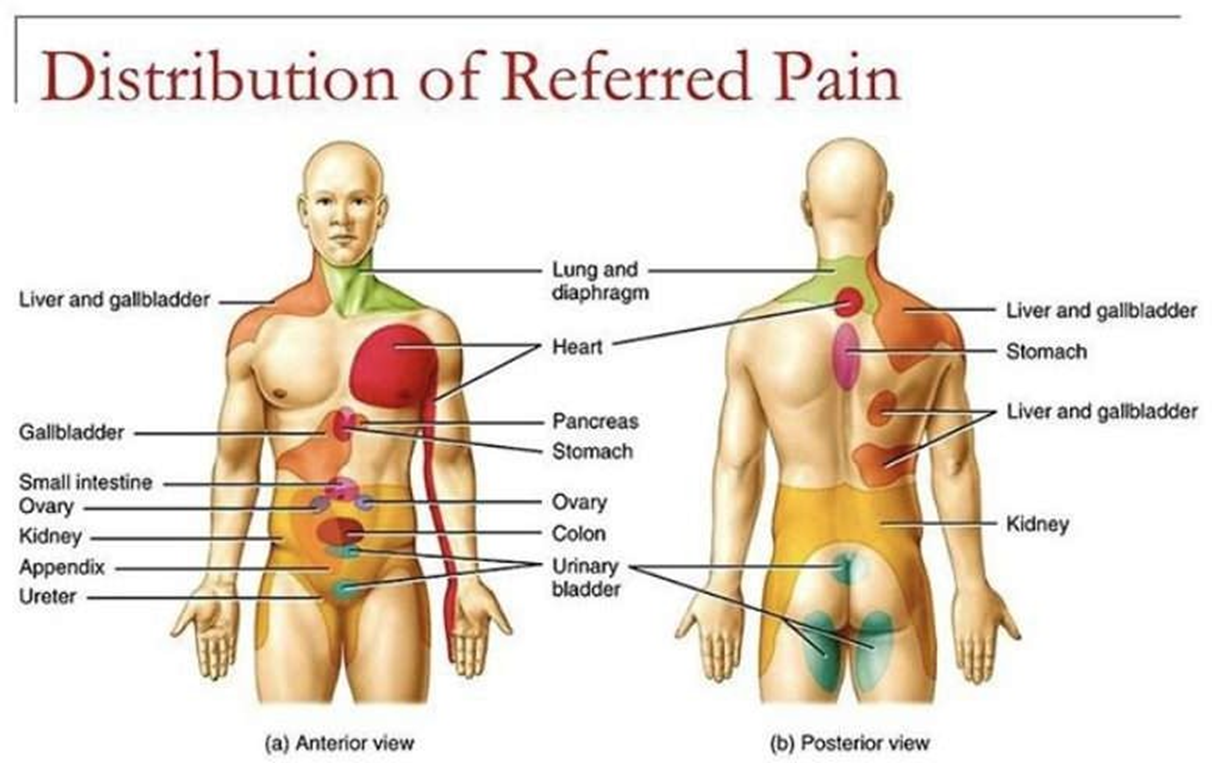
A patient is admitted for pain in the arm and jaw. The patient is later diagnosed with angina.
What type of pain does the arm and jaw pain most likely represent?
Explanation
Choice A rationale:
Intractable pain is pain that is persistent and does not respond to usual pain management methods. While angina can be intractable in some cases, it does not typically manifest as pain in the arm and jaw. Moreover, the patient in this scenario has not yet undergone pain management efforts, so it's premature to classify the pain as intractable.
Choice B rationale:
Phantom pain is pain that is felt in a part of the body that has been amputated or is no longer there. The patient in this scenario has not experienced any amputations, so phantom pain is not a valid explanation for the arm and jaw pain.
Choice C rationale:
Referred pain is pain that is felt in a part of the body that is different from the source of the pain. This is the most likely explanation for the arm and jaw pain in this patient. The heart and the arm and jaw share nerve pathways, so pain signals from the heart can be misinterpreted by the brain as coming from these other areas. This is a common phenomenon in patients with angina.
Choice D rationale:
Cramping pain is a type of pain that is often described as a muscle tightening or squeezing sensation. It is not typically associated with angina. While angina can sometimes cause chest tightness, it's not characterized by cramping in the arm and jaw.
A nurse is caring for a patient who is postoperative following a total knee replacement. What action should the nurse take to prevent deep vein thrombophlebitis?
Explanation
The correct answer is Choice A.
Choice A rationale: Encouraging increased fluid intake helps maintain blood volume and reduces viscosity, promoting circulation and lowering the risk of venous stasis and clot formation postoperatively.
Choice B rationale: Keeping the affected knee flexed impairs venous return and increases stasis, elevating the risk of thrombosis. Proper positioning with extension promotes circulation and reduces clot risk.
Choice C rationale: Prolonged bed rest contributes to immobility-induced venous stasis, a major risk factor for DVT. Early ambulation and leg exercises are essential to prevent thromboembolic events.
Choice D rationale: Massaging the calf of a postoperative patient is contraindicated due to the risk of dislodging a thrombus, potentially leading to a life-threatening pulmonary embolism.
A nurse enters a client’s room to answer the call light and finds the client on the bathroom floor. What should be the nurse’s initial action?
Explanation
The correct answer is choiceD.
Choice A rationale:
Assisting the client back into bed is not the initial action.Moving the client without assessing their condition could potentially cause harm.
Choice B rationale:
Notifying the client’s provider is important, but it should be done after assessing the client’s condition to provide accurate information.
Choice C rationale:
Informing the client’s family member is not the immediate priority.The nurse should first ensure the client’s safety and assess their condition.
Choice D rationale:
Obtaining the client’s vital signs is the initial action.This helps assess the client’s current condition and determine if there are any immediate medical needs.
Explanation
Rationale for Choice A: Obtain vital signs
While obtaining vital signs is important in assessing a patient's overall condition, it is not the first priority in a suspected transfusion reaction.
Vital signs can provide valuable information about the severity of the reaction, but they should not delay the immediate action of stopping the transfusion.
Delaying the cessation of the transfusion could allow for further infusion of incompatible blood or allergens, potentially worsening the reaction and leading to more serious complications.
Rationale for Choice B: Notify the registered nurse
Involving other healthcare professionals is crucial in managing transfusion reactions, but it should not precede stopping the transfusion.
The nurse should prioritize stopping the transfusion to prevent further exposure to potential triggers and then promptly notify the registered nurse for further assessment and interventions.
Timely communication with the registered nurse is essential for coordinating care and ensuring appropriate treatment measures are implemented.
Rationale for Choice C: Administer diphenhydramine
Diphenhydramine, an antihistamine, can be used to treat allergic reactions, but it should not be administered as the first response in this scenario.
The priority is to halt the infusion of the blood product that is potentially causing the reaction.
Administering diphenhydramine before stopping the transfusion could mask the symptoms of the reaction, making it more difficult to assess its severity and progression.
Rationale for Choice D: Stop the transfusion
This is the correct and most immediate action to take when a patient develops itching and hives during a blood transfusion.
These symptoms are indicative of a possible allergic or transfusion reaction, and stopping the transfusion is essential to prevent further complications.
It's critical to act quickly to minimize the amount of incompatible blood or allergens that enter the patient's circulation.
By stopping the transfusion, the nurse can potentially prevent the reaction from worsening and safeguard the patient's well- being.
Explanation
Choice A rationale:
Awaiting biopsy results can certainly cause anxiety and stress, but it doesn't directly impact the physiological mechanisms that modulate pain perception.
While a patient awaiting biopsy results may be more attentive to their bodily sensations, including pain, the anxiety itself is not the primary driver of a lowered pain threshold.
It's important to address the patient's concerns and provide emotional support, but this alone may not be sufficient to manage pain effectively if anxiety is not the primary factor.
Choice B rationale:
Anxiety activates the sympathetic nervous system, which triggers the "fight-or-flight" response. This cascade of physiological changes includes:
Increased heart rate and blood pressure Muscle tension
Dilated pupils
Heightened awareness of bodily sensations
These physiological changes can amplify pain signals and lower the pain threshold, meaning that a person who is anxious may perceive pain more intensely than someone who is calm and relaxed.
This is because anxiety can reduce the effectiveness of the body's natural pain-inhibiting mechanisms, such as the release of endorphins and serotonin.
Choice C rationale:
Difficulty sleeping can also contribute to pain, but its effect on pain threshold is less direct than that of anxiety. Sleep deprivation can lead to:
Increased irritability Decreased pain tolerance Impaired cognitive function
These factors can make it more difficult to cope with pain, but they don't directly lower the threshold at which pain signals are perceived.
Choice D rationale:
Pain threshold varies among individuals due to a variety of factors, including: Genetics
Past experiences with pain Psychological factors Cultural beliefs
Coping mechanisms
It is incorrect to assume that all patients who have had surgery will have the same pain threshold.
Explanation
Choice A rationale:
Chronic pain can manifest in various behavioral and physical symptoms, including restlessness, pacing, grimacing, and other facial expressions of pain. These behaviors are often unconscious attempts to cope with or distract from the pain.
They may also reflect the emotional distress that often accompanies chronic pain. Patients may feel frustrated, anxious, or even depressed due to the persistent nature of their pain and its impact on their lives.
It's crucial for nurses to recognize these behavioral signs of pain, as patients may not always readily report their pain verbally. By observing these behaviors, nurses can assess the patient's pain level more accurately and provide appropriate interventions.
Choice B rationale:
Chronic pain is defined as pain that persists for longer than three months, often for much longer. It is not limited and short in duration.
This distinguishes it from acute pain, which is typically associated with an injury or illness and resolves within a few days or weeks.
Choice C rationale:
While some patients with chronic pain may have physical signs of tissue injury, this is not always the case. Chronic pain can also be caused by nerve damage, inflammation, or changes in the central nervous system.
In some cases, the underlying cause of chronic pain may be unknown.
Choice D rationale:
Although chronic pain may not always cause a significant change in vital signs, it can still be a very real and debilitating experience for patients.
Vital signs, such as heart rate, blood pressure, and respiratory rate, are often more sensitive to acute pain.
Nurses should not rely solely on vital signs to assess chronic pain. Instead, they should consider the patient's self-report of pain, behavioral cues, and other factors.
You just viewed 10 questions out of the 53 questions on the Ati Rn Custom Med Surg Surgical Patient Proctored Exam Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

