A 30-year-old African American had surgery 6 months ago and the incision site is now raised, indurated, and shiny. This is most likely which type of tissue growth?
Melanoma
Keloid
Nevus
Angioma
The Correct Answer is B
A. Melanoma:
Melanoma is a type of skin cancer that arises from melanocytes, the cells that produce pigment (melanin) in the skin. Melanoma lesions are typically irregularly shaped, often asymmetrical, with varying shades of color (brown, black, tan, red, blue). They may have an uneven border and can evolve over time. Melanomas can be raised but are not typically described as indurated (firm) and shiny. They are also more commonly associated with changes in color, size, and shape.
B. Keloid:
A keloid is an abnormal overgrowth of scar tissue that extends beyond the boundaries of the original wound or incision site. Keloids are characterized by their raised appearance, firm or indurated texture, and shiny surface compared to the surrounding skin. They may also be darker than the surrounding skin due to increased collagen deposition. Keloids can develop months after an injury or surgery and are more common in individuals with darker skin tones, such as African Americans.
C. Nevus:
A nevus, commonly known as a mole or birthmark, is a benign growth of melanocytes or other skin cells. Nevus lesions can vary in appearance but are often flat or slightly raised, with a uniform color (brown, black, tan, or flesh-colored). They are usually not described as indurated or shiny. Nevus lesions can be present at birth (congenital nevus) or develop later in life (acquired nevus).
D. Angioma:
Angiomas are benign tumors that originate from blood vessels or lymphatic vessels. They can present as red or purplish raised lesions on the skin. Angiomas are typically not described as indurated or shiny. Common types of angiomas include cherry angiomas (small, red papules) and spider angiomas (red, spider-like lesions with central vessels).
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. Stop the infusion of IV fluids:
This action may be appropriate if there are signs of infiltration or extravasation, where the IV fluid leaks into the surrounding tissue instead of entering the vein. Stopping the infusion can help prevent further tissue damage and assess the extent of the infiltration.
B. Apply cold compresses to the IV site:
Cold compresses can help reduce swelling and discomfort at the IV site. This action may be appropriate if there are signs of local inflammation or mild irritation at the insertion site.
C. Elevate the extremity on a pillow:
Elevating the extremity can help reduce swelling and promote venous return. This action is beneficial if there is edema or localized swelling above the IV site.
D. Flush the catheter with normal saline:
Flushing the catheter with normal saline is not typically the initial action in response to edema and tenderness above the IV site. Flushing is more commonly performed to ensure patency and proper functioning of the IV catheter.
Correct Answer is D
Explanation
A. Excessive scarring:
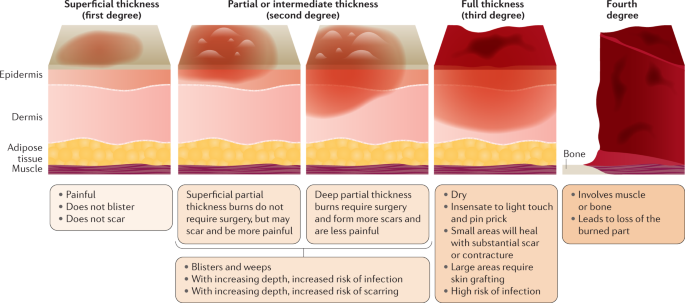
Excessive scarring is not an example of a first-degree burn. It typically occurs in more severe burns that affect deeper layers of the skin, such as second-degree or third-degree burns. Second-degree burns extend into the dermis, while third-degree burns damage all layers of the skin and can lead to significant scarring. First-degree burns, on the other hand, only affect the outer layer of the skin (epidermis) and usually do not result in excessive scarring.
B. Blistering from flames:
Blistering from flames is more characteristic of a second-degree burn rather than a first-degree burn. Second-degree burns involve damage to both the epidermis and part of the dermis, which can result in blister formation. These burns are often caused by direct contact with flames, hot liquids, or steam.
C. Blackened dead skin:
Blackened dead skin is indicative of a third-degree burn, which is the most severe type of burn. Third-degree burns damage all layers of the skin, including the epidermis, dermis, and sometimes underlying tissues. The skin may appear charred or blackened, and these burns often require medical intervention, such as skin grafting, due to the extent of tissue damage.
D. A sunburn:
A sunburn is an example of a first-degree burn. It occurs due to overexposure to ultraviolet (UV) radiation from the sun, leading to redness, pain, and mild swelling of the skin. First-degree burns affect only the outer layer of the skin (epidermis) and typically heal within a few days without significant scarring or blistering. Applying soothing lotions, staying hydrated, and avoiding further sun exposure can help manage sunburns.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today