A nurse is giving a preoperative patient a dose of famotidine ( Pepcid). The patient asks why the nurse is giving this drug when the patient has no history of ulcers. What response by the nurse is best?
“All preoperative patients get this medication."
“The physician prescribed this medication for you."
"It helps present ulcers from the stress of the surgery."
“Since you don't have ulcers, I will have to ask."
The Correct Answer is C
A. “All preoperative patients get this medication.” This statement is too broad and not entirely accurate. While many preoperative patients do receive famotidine (Pepcid), it’s not a standard for all. Medications are prescribed based on individual patient needs and medical history.
B. “The physician prescribed this medication for you.” While this is technically true, it doesn’t provide the patient with an understanding of why the medication is necessary. As a nurse, part of your role is to educate patients about their medications.
C. “It helps prevent ulcers from the stress of the surgery.” This is the correct answer. Famotidine (Pepcid) is given to decrease the amount of acid produced in the stomach, which can help prevent stress ulcers that can occur due to the physical stress of surgery.
D. “Since you don’t have ulcers, I will have to ask.” This statement suggests uncertainty and a lack of knowledge about the medication’s purpose. It’s important for healthcare professionals to understand the medications they administer and be able to explain them to patients.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
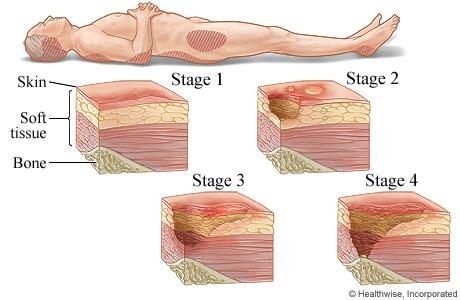
A. Stage III pressure injury
Stage III pressure injuries involve full-thickness skin loss, extending into the subcutaneous tissue but not through the fascia. These wounds typically present as deep craters and may involve undermining or tunneling. Non-blanchable erythema alone without visible skin loss is not characteristic of a Stage III pressure injury.
B. Stage IV pressure injury
Stage IV pressure injuries are the most severe and involve full-thickness tissue loss with exposed bone, tendon, or muscle. These wounds often have extensive tissue damage and can be difficult to manage. Again, non-blanchable erythema without visible skin loss is not indicative of a Stage IV pressure injury.
C. Stage II pressure injury
Stage II pressure injuries involve partial-thickness skin loss with damage to the epidermis and possibly the dermis. These wounds often present as shallow open ulcers or blisters and may have characteristics such as intact or ruptured blisters. While Stage II injuries can present with erythema, non-blanchable erythema specifically indicates a Stage I injury.
D. Stage I pressure injury
Stage I pressure injuries are the earliest stage and involve non-blanchable erythema of intact skin. The skin may be warmer or cooler than surrounding tissue and may have changes in sensation. There is no visible skin loss at this stage, but the area is at risk for further injury if pressure is not relieved. Therefore, non-blanchable erythema on the heels most likely indicates a Stage I pressure injury.
Correct Answer is C
Explanation
A. Inform the client that the recovery nurse will instruct them how to manage postoperative pain:
This is an important aspect of postoperative care, but it is typically addressed by the post-anesthesia care unit (PACU) or recovery nurse after surgery rather than in the preoperative education phase. While pain management education is crucial, the focus of preoperative education is usually on what to expect before, during, and immediately after surgery.
B. Remind the client they will return to their room after surgery:
This information is part of the preoperative instructions and helps alleviate anxiety by providing clarity about the post-surgical process. However, it may not be the most critical aspect of preoperative education compared to other options.
C. Provide instructions about how to cough and deep breathe effectively:
This is a key nursing intervention to include in preoperative education. Teaching the client how to cough and deep breathe effectively helps prevent postoperative complications such as atelectasis and pneumonia. These breathing techniques are typically taught preoperatively to ensure the client understands and can perform them correctly after surgery.
D. Notify the client that they will receive a food tray in the recovery room:
While it's important for the client to understand the postoperative diet plan, including any dietary restrictions or instructions, this information is usually provided after surgery rather than in the preoperative education phase.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today