A nurse cares for a patient who has a deep wound that is being treated with a wet to-damp (used to be dry) dressing. Which intervention would the nurse include in this patient’s plan of care?
Change the dressing when it is saturated.
Assess the wound bed once a day.
Contact the provider when the dressing leaks.
Change the dressing every 6 hours.
The Correct Answer is A
A. Change the dressing when it is saturated:
This intervention is the most appropriate for managing a deep wound with a wet to-damp dressing. Wet to-damp dressings are designed to maintain a moist environment conducive to wound healing. Changing the dressing when it becomes saturated with wound exudate helps prevent excessive moisture accumulation, which can lead to skin maceration and potential infection. It ensures that the wound bed remains in an optimal healing environment and reduces the risk of complications.
B. Assess the wound bed once a day:
Assessing the wound bed is an essential part of wound care, as it allows the nurse to monitor healing progress, assess for signs of infection, and evaluate the effectiveness of the chosen dressing. However, the frequency of wound bed assessment may vary depending on the specific patient's needs and the type of dressing being used. While daily assessment is generally recommended, it does not directly dictate the timing of dressing changes for wet to-damp dressings, which are primarily changed based on saturation levels.
C. Contact the provider when the dressing leaks:
Contacting the provider when the dressing leaks or when there are concerns or complications is an important step in patient care. Leaking dressings can indicate issues with the dressing application, excessive wound exudate, or potential complications such as infection. It's crucial to inform the provider promptly so that appropriate interventions can be implemented, but this instruction is more reactive and does not specifically address the timing of dressing changes.
D. Change the dressing every 6 hours:
Changing the dressing every 6 hours is not typically recommended for wet to-damp dressings unless specifically indicated based on the patient's condition and the amount of wound exudate. Frequent dressing changes can disrupt the healing process, cause unnecessary trauma to the wound bed, and increase the risk of infection. Dressing change frequency should be based on the assessment of wound exudate and the dressing's ability to maintain a moist environment.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
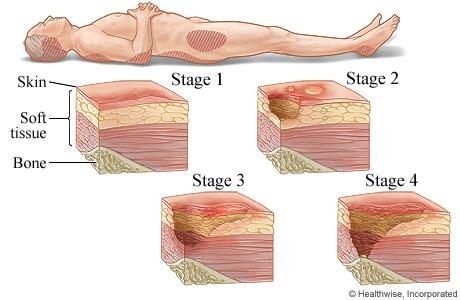
A. Stage III pressure injury
Stage III pressure injuries involve full-thickness skin loss, extending into the subcutaneous tissue but not through the fascia. These wounds typically present as deep craters and may involve undermining or tunneling. Non-blanchable erythema alone without visible skin loss is not characteristic of a Stage III pressure injury.
B. Stage IV pressure injury
Stage IV pressure injuries are the most severe and involve full-thickness tissue loss with exposed bone, tendon, or muscle. These wounds often have extensive tissue damage and can be difficult to manage. Again, non-blanchable erythema without visible skin loss is not indicative of a Stage IV pressure injury.
C. Stage II pressure injury
Stage II pressure injuries involve partial-thickness skin loss with damage to the epidermis and possibly the dermis. These wounds often present as shallow open ulcers or blisters and may have characteristics such as intact or ruptured blisters. While Stage II injuries can present with erythema, non-blanchable erythema specifically indicates a Stage I injury.
D. Stage I pressure injury
Stage I pressure injuries are the earliest stage and involve non-blanchable erythema of intact skin. The skin may be warmer or cooler than surrounding tissue and may have changes in sensation. There is no visible skin loss at this stage, but the area is at risk for further injury if pressure is not relieved. Therefore, non-blanchable erythema on the heels most likely indicates a Stage I pressure injury.
Correct Answer is ["A","D","E"]
Explanation
A. Decreased plasma volume:Burn injuries cause a significant inflammatory response, leading to fluid shifts from the intravascular space to the interstitial space. This results in hypovolemia and decreased plasma volume, especially during the acute phase of burns.
B. Diuresis:Diuresis typically occurs after fluid resuscitation and stabilization of the client (in the later phase of burn recovery). In the initial phase, oliguria is more common due to hypovolemia and reduced renal perfusion.
C. Hypermagnesemia:Hypermagnesemia is not typically associated with burn injuries. Instead, clients with burns often experience hypomagnesemia due to fluid shifts, protein loss, and increased renal losses.
D. Capillary leak:Burn injuries lead to a systemic inflammatory response, causing capillary leak syndrome. This increases vascular permeability, allowing fluid, electrolytes, and proteins to leak into the interstitial spaces, contributing to edema and hypovolemia.
E. Loss of protein:Proteins are lost through damaged capillaries and open burn wounds, contributing to decreased oncotic pressure, edema, and a need for aggressive nutritional support to promote healing and recovery.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today