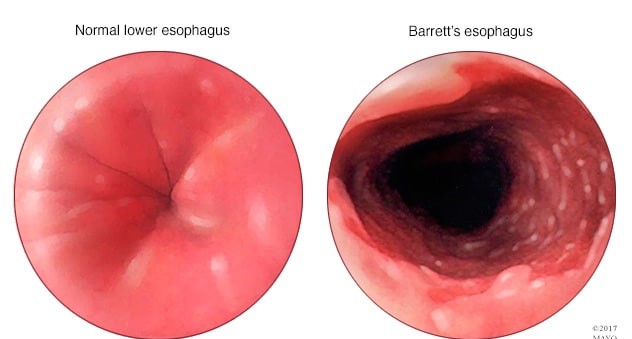
A client diagnosed with Barrett's esophagus asks how he developed this. Which of the following responses by the nurse is most accurate?
"Your allergies have most likely contributed to this."
"Your history of gastroesophageal reflux disorder is the most likely cause."
"Being a vegetarian has caused an imbalance in stomach acid."
"This is a genetic condition that you were born with."
The Correct Answer is B
Choice A reason: This is incorrect because allergies are not a risk factor for developing Barrett's esophagus. Allergies are hypersensitive reactions of the immune system to certain substances, such as pollen, dust, or food. They can cause symptoms such as sneezing, itching, or hives, but they do not affect the esophagus or stomach acid.
Choice B reason: This is the correct answer because gastroesophageal reflux disorder (GERD) is the most common risk factor for developing Barrett's esophagus. GERD is a condition where the lower esophageal sphincter (LES) does not close properly and allows stomach acid to flow back into the esophagus. This can cause inflammation, irritation, and damage to the esophageal lining. Over time, this can lead to changes in the cells of the esophagus, which is called Barrett's esophagus.
Choice C reason: This is incorrect because being a vegetarian is not a risk factor for developing Barrett's esophagus. Being a vegetarian means avoiding meat and animal products in the diet. This can have health benefits such as lower cholesterol and blood pressure levels, but it does not affect the esophagus or stomach acid.
Choice D reason: This is incorrect because Barrett's esophagus is not a genetic condition that one is born with. Barrett's esophagus is an acquired condition that results from chronic exposure to stomach acid in the esophagus. It is not inherited from one's parents or passed on to one's children.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because encouraging coughing and deep breathing can increase intracranial pressure (ICP), which is the pressure inside
the skull that can affect brain function. Coughing and deep breathing can increase blood flow and oxygen demand to the brain, which can worsen cerebral edema. The nurse should suction the patient as needed and maintain a patent airway.
Choice B Reason: This is incorrect because positioning the patient with knees and hips flexed can increase ICP by reducing venous drainage from the head. The nurse should position the patient with neck and body in alignment and avoid extreme flexion or extension of any joints.
Choice C Reason: This is incorrect because performing nursing interventions once an hour can disturb the patient's sleep and increase ICP by stimulating brain activity. The nurse should cluster nursing interventions and provide quiet and dark environment to promote rest and reduce stress.
Choice D Reason: This is correct because keeping the head of the bed elevated to 30 degrees can decrease ICP by facilitating venous drainage from the head and reducing cerebral blood volume. The nurse should monitor the patient's blood pressure and pulse to ensure adequate cerebral perfusion.
Correct Answer is C
Explanation
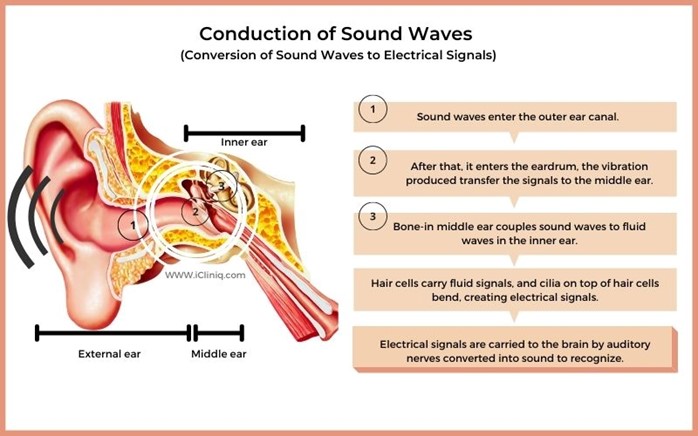
Choice A reason: This is incorrect because using sign language when communicating with the client is not an appropriate action for the nurse to take. Sign language is a form of communication that uses hand gestures, facial expressions, and body movements. It is not a universal language and requires training and practice. The nurse should not assume that the client knows or prefers sign language unless they have indicated so.
Choice B reason: This is incorrect because speaking loudly and into the client's good ear is not an appropriate action for the nurse to take. Speaking loudly can distort the sound quality and cause discomfort or irritation to the client. Speaking into the client's good ear can also create a sense of imbalance and isolation. The nurse should speak at a normal volume and tone, and face the client directly.
Choice C reason: This is the correct answer because speaking directly to the client in a normal, clear voice is an appropriate action for the nurse to take. Speaking directly to the client can help them see the nurse's mouth movements and facial expressions, which can enhance understanding and communication. Speaking in a normal, clear voice can help convey the message clearly and respectfully.
Choice D reason: This is incorrect because sitting by the client's side and speaking very slowly is not an appropriate action for the nurse to take. Sitting by the client's side can make it difficult for them to see the nurse's face and hear their voice. Speaking very slowly can also make the message unclear and patronizing. The nurse should sit in front of the client and speak at a normal pace.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today