A client is being discharged with a prescription for warfarin. Which instruction should the nurse provide this client regarding diet?
Increase the intake of dark green leafy vegetables while taking warfarin.
Eat two servings of dark green leafy vegetables daily and continue for 30 days after warfarin therapy is completed.
Eat approximately the same amount of leafy green vegetables daily so the amount of vitamin K consumed is consistent.
Avoid eating any foods that contain any vitamin K because it is an antagonist of warfarin.
The Correct Answer is C
Choice A reason: Increasing the intake of dark green leafy vegetables while taking warfarin is not a good instruction because it can decrease the effectiveness of warfarin. Dark green leafy vegetables are rich in vitamin K, which is a coagulation factor that counteracts the anticoagulant effect of warfarin.
Choice B reason: Eating two servings of dark green leafy vegetables daily and continuing for 30 days after warfarin therapy is completed is not a good instruction because it can cause bleeding complications. Dark green leafy vegetables are rich in vitamin K, which is a coagulation factor that counteracts the anticoagulant effect of warfarin. Stopping warfarin while continuing to eat high amounts of vitamin K can increase the risk of clot formation and thromboembolism.
Choice D reason: Avoiding eating any foods that contain any vitamin K because it is an antagonist of warfarin is not a good instruction because it can cause bleeding complications. Dark green leafy vegetables are rich in vitamin K, which is a coagulation factor that counteracts the anticoagulant effect of warfarin. Eliminating vitamin K from the diet can increase the sensitivity to warfarin and cause excessive bleeding and bruising.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: Support stockings may help with peripheral edema, but they are not the priority intervention for this client. The client's low serum albumin level indicates malnutrition and increased risk of infection and poor wound healing.
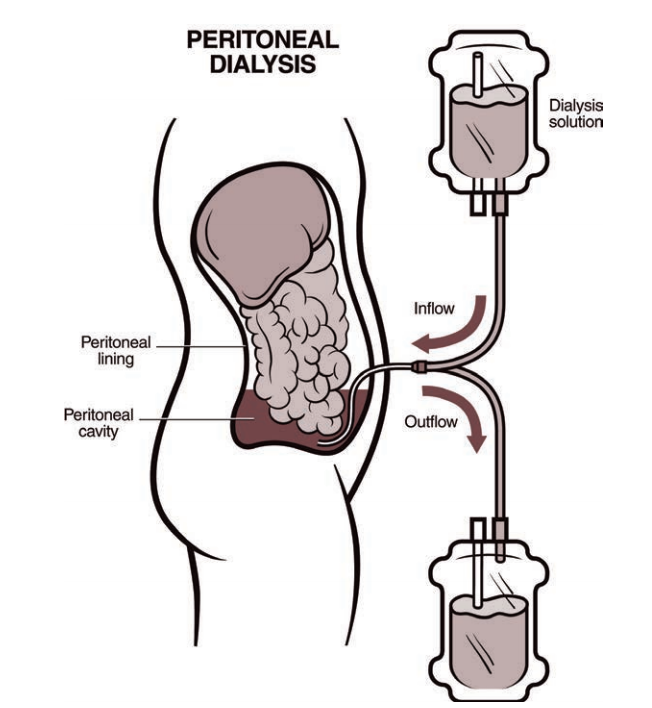
Choice C reason: Evaluating patency of the AV graft is not the priority intervention for this client because the client is receiving peritoneal dialysis, not hemodialysis. The AV graft may be used in the future if peritoneal dialysis fails, but it is not an immediate concern.
Choice D reason: Instructing the client to follow fluid restriction amounts is important for peritoneal dialysis patients, but it is not the priority intervention for this client. The client's low serum albumin level indicates that fluid restriction alone is not sufficient to manage fluid balance and prevent edema.
Correct Answer is ["A","B","E"]
Explanation
Choice C reason: Initiating patient controlled analgesia (PCA. pumps for two clients immediately postoperatively is not a nursing action that can be assigned to the PN. PCA pump is a device that allows the client to self-administer pain medication through an IV line by pressing a button. PCA pump should be initiated by the nurse after verifying the prescription, setting the parameters, educating the client, and ensuring safety and effectiveness. The PN does not have the authority or competency to initiate PCA pump or adjust its settings.
Choice D reason: Starting the second blood transfusion for a client twelve hours following a below knee amputation is not a nursing action that can be assigned to the PN. Blood transfusion is a procedure that delivers donated blood or blood products into the client's bloodstream through an IV line. Blood transfusion should be started by the nurse after verifying the prescription, checking the blood type and compatibility, obtaining informed consent, and monitoring for any adverse reactions. The PN does not have the authority or competency to start blood transfusion or manage its complications.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today