A client is scheduled for a routine physical assessment at the neighborhood clinic. What should the nurse do when physically assessing the client's oxygenation status? Select all that apply.
Observe for signs and symptoms of respiratory distress.
Auscultate anterior and posterior lung fields.
Inspect the skin for pallor and cyanosis.
Assess the shape, expansion, and symmetry of the chest.
Observe rate, rhythm, and depth of respirations.
Correct Answer : A,B,C,E
A. Observe for signs and symptoms of respiratory distress.
B. Auscultate anterior and posterior lung fields.
C. Inspect the skin for pallor and cyanosis.
E. Observe rate, rhythm, and depth of respirations.
When assessing a client's oxygenation status, a nurse should observe for signs and symptoms of respiratory distress, such as dyspnea, wheezing, and use of accessory muscles. Auscultation of the anterior and posterior lung fields is important to identify any adventitious breath sounds such as crackles, wheezes or rhonchi that may indicate airway obstruction, fluid accumulation, or other respiratory abnormalities. Inspection of the skin is also important to detect pallor or cyanosis, which may indicate reduced oxygen levels in the blood. Lastly, observing the rate, rhythm, and depth of respirations can provide information on the adequacy of oxygen exchange in the lungs.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","C","E"]
Explanation
The correct answer is choices A, C, and E.
- Stool is hard and has a consistency of small marbles is a sign of constipation.
- Bowel sounds that are hyperactive in all four quadrants are an indication of diarrhea rather than constipation.
- Client reports they have not had a bowel movement for the past 4 days supports the diagnosis of constipation.
- Client reports urgency when needing to have a bowel movement is more indicative of diarrhea than constipation.
- Client states they have to strain hard when having a bowel movement is a sign of constipation.
Correct Answer is C
Explanation
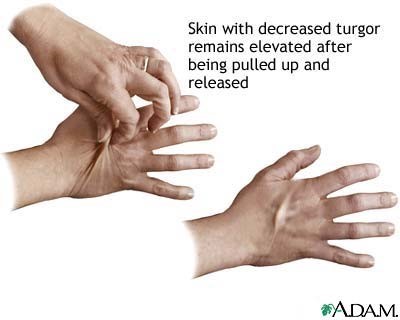
The correct answer is choice C: Skin fold returns to its usual shape quickly when released. When assessing skin turgor, the nurse is checking for the elasticity and hydration of the skin. In a normal assessment, when the skin fold is lifted or pinched, it should return to its usual shape quickly when released. This indicates good skin turgor, which is an indication of proper hydration. If the skin fold is difficult to lift or pinch (choice A), this indicates poor skin turgor and possible dehydration. If an indentation of 2 mm remains after releasing the skin fold (choice B), this indicates poor skin turgor and possible dehydration. If the skin fold returns to its usual shape slowly when released (choice D), this may indicate a decrease in skin elasticity and possible dehydration.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today