A client with a history of anxiety and depression presents to the emergency department with a headache, nausea, and vomiting. The client's vital signs are temperature 100.9°F (38.3°C), heart rate 115 beats/minute, respirations 21 breaths/minute, and blood pressure 216/108 mm Hg. When reviewing the client's medications, which information is of most concern to the nurse?
Hydrochlorothiazide 12.5 mg PO daily.
Phenelzine 60 mg PO daily.
Losartan 50 mg PO daily.
Aspirin 81 milligrams PO daily.
The Correct Answer is B
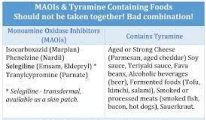
Choice A rationale: Hydrochlorothiazide is a diuretic and may contribute to electrolyte imbalances, but it is not the most concerning medication in this situation. Choice B rationale: Phenelzine is a monoamine oxidase inhibitor (MAOI), and the combination of an MAOI with certain foods or medications containing tyramine can lead
to a hypertensive crisis. The client's elevated blood pressure is of concern, and the nurse should notify the healthcare provider.
Choice C rationale: Losartan is an angiotensin II receptor blocker (ARB) used to treat hypertension. While it may contribute to blood pressure control, it is not the most concerning medication in this scenario.
Choice D rationale: Aspirin, at a dose of 81 milligrams, is often used for cardiovascular prophylaxis and is not the most concerning medication in this situation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A rationale: Changes in thought patterns related to problem-solving demonstrate the effectiveness of cognitive-behavioral techniques. Shifting from hopelessness to active problem-solving reflects positive progress.
Choice B rationale: Describing how the family can resolve problems may involve other therapeutic modalities, but it is not specific to evaluating the effectiveness of cognitive behavioral techniques.
Choice C rationale: Relating insight into problematic relationships is a broad goal and may not specifically measure the impact of cognitive-behavioral techniques. Choice D rationale: Demonstrating a healthy relationship with the husband is an important goal but is not directly related to the evaluation of cognitive-behavioral techniques.
Correct Answer is D
Explanation
Choice A rationale: "I know that bathing helps prevent infectious diseases" is a factual statement but may not necessarily reflect progress in the client's overall functioning and engagement in self-care. It focuses on the practical aspect of bathing rather than the client's motivation and insight.
Choice B rationale: "Others say I am dirty and smell badly, so I will bathe" suggests an external motivation rather than intrinsic motivation. Progress is better indicated when the client expresses a personal desire to engage in self-care activities.
Choice C rationale: "I will take a bath today as requested" indicates compliance with external requests rather than an internal desire to care for oneself. It is essential to foster the client's intrinsic motivation for self-care.
Choice D rationale: "I feel good when I take care of myself" reflects an internal motivation and positive reinforcement associated with self-care. This statementsuggests progress in the client's willingness to engage in personal hygiene activities.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today