A nurse collects the health history of a 65-year-old client. Which of the following risk factors in the client's history puts the client at the highest risk for embolic stroke?
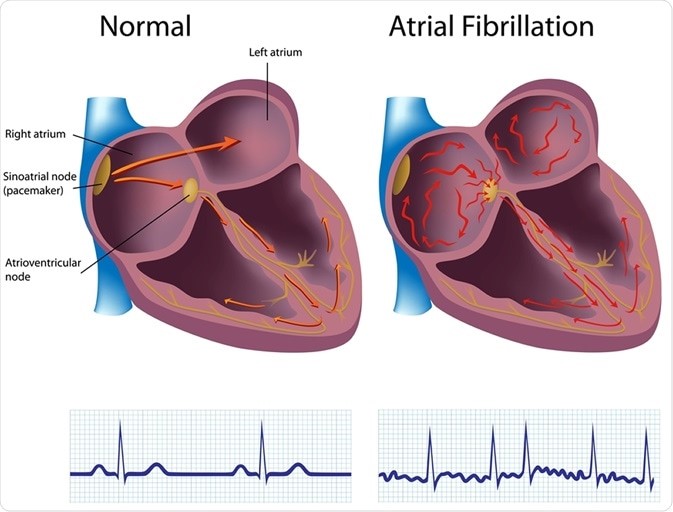
Atrial fibrillation.
Hypertension.
Diabetes.
Alcohol abuse.
The Correct Answer is A
Choice A reason: This is the correct answer because atrial fibrillation is the risk factor that puts the client at
the highest risk for embolic stroke. Atrial fibrillation is an irregular and rapid heart rate that causes poor blood flow and blood pooling in the heart chambers. This can lead to the formation of blood clots that can travel to the brain and block an artery, causing an embolic stroke.
Choice B reason: This is incorrect because hypertension is not the risk factor that puts the client at
the highest risk for embolic stroke. Hypertension is high blood pressure that puts stress on the blood vessels and increases the risk of bleeding or rupture. This can lead to a hemorrhagic stroke, but not an embolic stroke.
Choice C reason: This is incorrect because diabetes is not the risk factor that puts the client at
the highest risk for embolic stroke. Diabetes is a condition that causes high blood sugar levels and damages the blood vessels and nerves. This can lead to poor circulation and increased risk of infection and ulcers, but not an embolic stroke.
Choice D reason: This is incorrect because alcohol abuse is not the risk factor that puts the client at
the highest risk for embolic stroke. Alcohol abuse is excessive consumption of alcohol that affects liver function and blood clotting factors. This can lead to liver disease and bleeding disorders, but not an embolic stroke.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: This is correct because resuming a functional role in society is the ultimate goal for a client in the rehabilitative phase of a burn injury. The rehabilitative phase begins when wound healing is complete and lasts until physical and psychosocial recovery is achieved. The nurse should help the client regain independence, self-esteem, and quality of life by providing education, counseling, referrals, and resources.
Choice B reason: This is incorrect because pain management is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Pain management is important throughout all phases of burn care, but especially during wound healing and scar formation, which can cause itching, tightness, or hypersensitivity. The nurse should assess the client's pain level and administer analgesics, antipruritics, or moisturizers as ordered.
Choice C reason: This is incorrect because providing continued full support to the client is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Providing continued full support to the client can help them cope with physical and emotional challenges, such as scarring, disfigurement, disability, or depression. The nurse should provide emotional support, active listening, positive feedback, and encouragement to the client.
Choice D reason: This is incorrect because preventing infection is not a goal, but an intervention for a client in the rehabilitative phase of a burn injury. Preventing infection is crucial during wound healing and grafting, which can be compromised by bacterial colonization or contamination. The nurse should monitor the client's vital signs, wound appearance, and laboratory results, and administer antibiotics or antiseptics as ordered.
Correct Answer is D
Explanation
Choice A Reason: Decreased thickness of tympanic membranes is not a physiological change to hearing in older adult clients. The tympanic membranes are thin and flexible structures that vibrate in response to sound waves. The thickness of the tympanic membranes does not change significantly with age.
Choice B Reason: Decreased tinnitus is not a physiological change to hearing in older adult clients. Tinnitus is a ringing or buzzing sound in the ears that may be caused by various factors, such as noise exposure, ear infections, medications, or aging. Tinnitus may increase or decrease with age, depending on the underlying cause.
Choice C Reason: Decreased ear wax is not a physiological change to hearing in older adult clients. Ear wax is a natural substance that lubricates and protects the ear canal from dust, bacteria, and insects. Ear wax production may vary with age, but it does not affect hearing unless it accumulates and blocks the ear canal.
Choice D Reason: Decreased ability to hear high-frequency sounds is a physiological change to hearing in older adult clients. This is also known as presbycusis, which is a gradual loss of hearing that occurs as part of aging. Presbycusis affects the ability to hear high-pitched sounds, such as consonants, birdsong, or alarms.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today