A nurse enters the room of a client and discovers the client with new right-sided weakness and slurred speech. Which of the following actions should the nurse take?
Perform carotid massage.
Call for help.
Provide the client with water to test the gag reflex.
Administer thrombolytics.
The Correct Answer is B
Choice A reason: Performing carotid massage is not an appropriate action for a nurse to take when a client has signs of a stroke, as it may worsen the condition or cause complications. Carotid massage is a technique that involves applying pressure to the carotid artery in the neck to stimulate the vagus nerve and slow down the heart rate. It is used to treat some types of arrhythmias, such as supraventricular tachycardia. However, carotid massage may dislodge a blood clot or plaque from the carotid artery and cause an embolic stroke, which is a type of ischemic stroke that occurs when a blood clot travels to the brain and blocks a blood vessel. Carotid massage may also cause bradycardia, hypotension, or syncope, which can reduce the blood flow to the brain and worsen the ischemic damage.
Choice B reason: Calling for help is an appropriate action for a nurse to take when a client has signs of a stroke, as it initiates the emergency response and allows for prompt evaluation and treatment. Stroke is a medical emergency that occurs when the blood supply to a part of the brain is interrupted, causing brain cells to die. The sooner the stroke is recognized and treated, the better the chances of survival and recovery. Therefore, the nurse should call for help as soon as possible and activate the stroke protocol in the facility.
Choice C reason: Providing the client with water to test the gag reflex is not an appropriate action for a nurse to take when a client has signs of a stroke, as it may cause aspiration or choking. A gag reflex is an involuntary contraction of the throat muscles that prevents foreign objects from entering the airway. It is tested by touching the back of the throat with a tongue depressor or a cotton swab. However, this test is not indicated in a client who has signs of a stroke, as it may trigger vomiting or coughing, which can increase intracranial pressure or cause bleeding. Moreover, giving water to a client who has signs of a stroke may be dangerous, as they may have dysphagia (difficulty swallowing) or facial weakness, which can impair their ability to swallow safely and increase the risk of aspiration pneumonia.
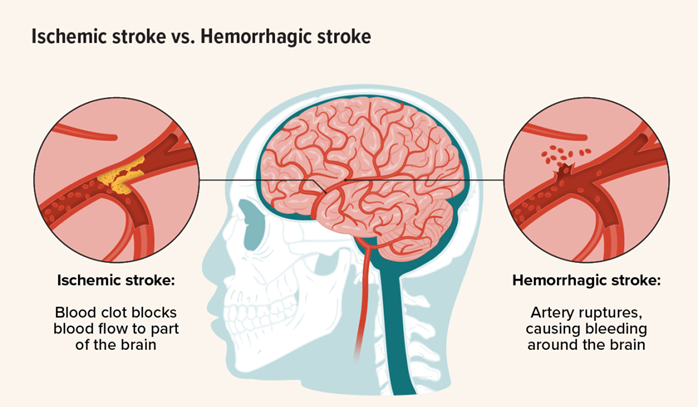
Choice D reason: Administering thrombolytics is not an appropriate action for a nurse to take when a client has signs of a stroke, as it may be contraindicated or harmful depending on the type and timing of the stroke. Thrombolytics are medications that dissolve blood clots and restore blood flow. They are used to treat ischemic stroke, which is caused by a blood clot that blocks a blood vessel in the brain. However, thrombolytics are not effective for hemorrhagic stroke, which is caused by bleeding into or around the brain. In fact, thrombolytics may worsen hemorrhagic stroke by increasing bleeding and intracranial pressure. Therefore, thrombolytics should only be given after confirming the type of stroke by imaging tests such as computed tomography (CT) scan or magnetic resonance imaging (MRI). Thrombolytics should also be given within a specific time window after the onset of symptoms, usually within 3 to 4.5 hours, as they may lose their effectiveness or cause complications if given too late. Therefore, administering thrombolytics is not an action that a nurse can take without proper assessment and orders from the health care provider.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Monitoring vital signs and neurological status frequently is a priority intervention for a client who has experienced a hemorrhagic stroke, as it helps to detect any changes in the client's condition and guide appropriate treatment. Hemorrhagic stroke is a medical emergency that occurs when a blood vessel in the brain ruptures and causes bleeding into the brain tissue. This can lead to increased intracranial pressure, cerebral edema, and brain damage. Therefore, the nurse should monitor the client's blood pressure, pulse, respiration, temperature, level of consciousness, pupil reaction, motor function, and sensory function frequently and report any abnormalities to the health care provider.
Choice B reason: Maintaining strict bed rest to minimize cerebral blood flow is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may not prevent further bleeding or improve the client's outcome. In fact, strict bed rest may increase the risk of complications such as deep vein thrombosis, pulmonary embolism, pneumonia, pressure ulcers, and muscle atrophy. The nurse should follow the health care provider's orders regarding the client's activity level and position. The nurse should also provide adequate hydration, nutrition, skin care, and comfort measures to the client.
Choice C reason: Administering anticoagulant medications as prescribed is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may worsen the bleeding and increase the risk of intracranial hemorrhage. Anticoagulant medications are used to prevent or treat ischemic stroke, which is caused by a blood clot that blocks a blood vessel in the brain. However, anticoagulant medications are contraindicated in hemorrhagic stroke, as they interfere with the blood's ability to clot and stop the bleeding. The nurse should avoid giving any medications that may affect coagulation or platelet function to the client unless ordered by the health care provider.
Choice D reason: Assisting the client with active range of motion exercises is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may not improve the client's neurological function or prevent complications. Active range of motion exercises are performed by the client with or without assistance from the nurse to maintain joint mobility and muscle strength. However, these exercises are not indicated in the acute phase of hemorrhagic stroke, as they may increase intracranial pressure or cause pain or discomfort to the client. The nurse should consult with the physical therapist before initiating any exercise program for the client.
Correct Answer is B
Explanation
Choice A reason: Performing carotid massage is not an appropriate action for a nurse to take when a client has signs of a stroke, as it may worsen the condition or cause complications. Carotid massage is a technique that involves applying pressure to the carotid artery in the neck to stimulate the vagus nerve and slow down the heart rate. It is used to treat some types of arrhythmias, such as supraventricular tachycardia. However, carotid massage may dislodge a blood clot or plaque from the carotid artery and cause an embolic stroke, which is a type of ischemic stroke that occurs when a blood clot travels to the brain and blocks a blood vessel. Carotid massage may also cause bradycardia, hypotension, or syncope, which can reduce the blood flow to the brain and worsen the ischemic damage.
Choice B reason: Calling for help is an appropriate action for a nurse to take when a client has signs of a stroke, as it initiates the emergency response and allows for prompt evaluation and treatment. Stroke is a medical emergency that occurs when the blood supply to a part of the brain is interrupted, causing brain cells to die. The sooner the stroke is recognized and treated, the better the chances of survival and recovery. Therefore, the nurse should call for help as soon as possible and activate the stroke protocol in the facility.
Choice C reason: Providing the client with water to test the gag reflex is not an appropriate action for a nurse to take when a client has signs of a stroke, as it may cause aspiration or choking. A gag reflex is an involuntary contraction of the throat muscles that prevents foreign objects from entering the airway. It is tested by touching the back of the throat with a tongue depressor or a cotton swab. However, this test is not indicated in a client who has signs of a stroke, as it may trigger vomiting or coughing, which can increase intracranial pressure or cause bleeding. Moreover, giving water to a client who has signs of a stroke may be dangerous, as they may have dysphagia (difficulty swallowing) or facial weakness, which can impair their ability to swallow safely and increase the risk of aspiration pneumonia.
Choice D reason: Administering thrombolytics is not an appropriate action for a nurse to take when a client has signs of a stroke, as it may be contraindicated or harmful depending on the type and timing of the stroke. Thrombolytics are medications that dissolve blood clots and restore blood flow. They are used to treat ischemic stroke, which is caused by a blood clot that blocks a blood vessel in the brain. However, thrombolytics are not effective for hemorrhagic stroke, which is caused by bleeding into or around the brain. In fact, thrombolytics may worsen hemorrhagic stroke by increasing bleeding and intracranial pressure. Therefore, thrombolytics should only be given after confirming the type of stroke by imaging tests such as computed tomography (CT) scan or magnetic resonance imaging (MRI). Thrombolytics should also be given within a specific time window after the onset of symptoms, usually within 3 to 4.5 hours, as they may lose their effectiveness or cause complications if given too late. Therefore, administering thrombolytics is not an action that a nurse can take without proper assessment and orders from the health care provider.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today