A nurse in the emergency department is caring for a client who has an epidural hematoma following a motor-vehicle crash. Which of the following is an expected finding for this client?
Drainage of clear fluid from the ears
Alternating periods of alertness and unconsciousness
Narrowing pulse pressure
Extensive bruising in the mastoid area
The Correct Answer is B
Choice A: Drainage of clear fluid from the ears is not an expected finding for a client who has an epidural hematoma, but rather a sign of a basilar skull fracture, which is a different type of head injury. The clear fluid is cerebrospinal fluid (CSF), which leaks from the brain through the fractured skull.
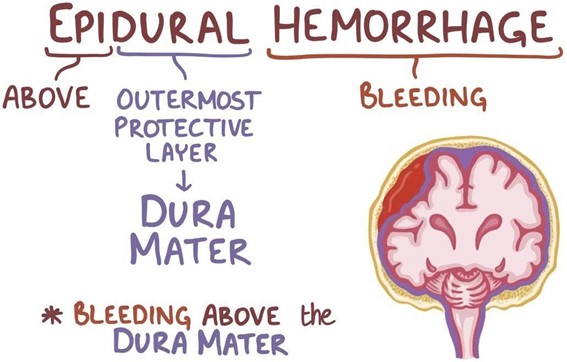
Choice B: Alternating periods of alertness and unconsciousness is an expected finding for a client who has an epidural hematoma, because it indicates a rapid increase in intracranial pressure (ICP) due to bleeding between the dura mater and the skull. The client may have a brief loss of consciousness at the time of injury, followed by a lucid interval, and then a rapid deterioration of mental status.
Choice C: Narrowing pulse pressure is not an expected finding for a client who has an epidural hematoma, but rather a sign of increased ICP due to any cause. Pulse pressure is the difference between systolic and diastolic blood pressure. As ICP rises, it compresses the brainstem and causes bradycardia and hypertension, resulting in a decreased pulse pressure.
Choice D: Extensive bruising in the mastoid area is not an expected finding for a client who has an epidural hematoma, but rather a sign of a basilar skull fracture, which is a different type of head injury. The bruising is also known as Batle's sign, and it occurs due to blood pooling behind the ear.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: Urine output is not a finding that should decrease with adequate fluid replacement. On the contrary, urine output should increase as the fluid therapy restores the renal perfusion and function. The nurse should monitor the urine output and ensure that it is at least 0.5 mL/kg/hr for adults and 1 mL/kg/hr for children.
Choice B Reason: Heart rate is a finding that should decrease with adequate fluid replacement. A high heart rate is a sign of hypovolemia, which occurs when the burn injury causes fluid loss from the intravascular space. The nurse should monitor the heart rate and expect it to decrease as the fluid therapy replenishes the blood volume and improves the cardiac output.
Choice C Reason: Weight is not a finding that should decrease with adequate fluid replacement. On the contrary, weight may increase as the fluid therapy restores the hydration status and corrects the fluid deficit. The nurse should monitor the weight and compare it with the pre-burn weight to evaluate the fluid balance.
Choice D Reason: Blood pressure is not a finding that should decrease with adequate fluid replacement. On the contrary, blood pressure may increase as the fluid therapy restores the vascular tone and improves the tissue perfusion. The nurse should monitor the blood pressure and expect it to increase as the fluid therapy compensates for the fluid loss.
Correct Answer is D
Explanation
Choice A Reason: This choice is incorrect because warm, flushed skin is not a sign of respiratory acidosis. Warm, flushed skin may indicate fever, infection, inflammation, or allergic reaction, but it does not reflect the acid-base imbalance in the blood.
Choice B Reason: This choice is incorrect because hyperactive deep tendon reflexes are not a sign of respiratory acidosis. Hyperactive deep tendon reflexes may indicate hypocalcemia, hyperthyroidism, or spinal cord injury, but they do not reflect the carbon dioxide level in the blood.
Choice C Reason: This choice is incorrect because bounding peripheral pulses are not a sign of respiratory acidosis. Bounding peripheral pulses may indicate increased cardiac output, anxiety, or hyperthyroidism, but they do not reflect the pH level in the blood.
Choice D Reason: This choice is correct because widened QRS complexes are a sign of respiratory acidosis. QRS complexes are the segments on an electrocardiogram (ECG) that represent the depolarization of the ventricles. A normal QRS complex duration is 0.06 to 0.10 seconds, and a widened QRS complex duration is more than 0.12 seconds. A widened QRS complex may indicate hyperkalemia, which is a common complication of kidney failure and respiratory acidosis. Hyperkalemia is a condition in which the serum potassium level is higher than normal (more than 5 mEq/L). It may cause cardiac arrhythmias, muscle weakness, or paralysis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today