A nurse is assessing a full-term newborn upon admission to the nursery. Which of the following clinical findings should the nurse report to the provider?
Rust-stained urine.
Single palmar creases.
Subconjunctival hemorrhage.
Transient circumoral cyanosis
The Correct Answer is B
The correct answer is choice B. Single palmar creases.
Choice A rationale:
Rust-stained urine is typically due to urate crystals and is common in newborns. It usually resolves on its own and is not a cause for concern.
Choice B rationale:
Single palmar creases can be associated with certain genetic conditions, such as Down syndrome. This finding should be reported to the provider for further evaluation.
Choice C rationale:
Subconjunctival hemorrhage is a common finding in newborns due to the pressure changes during delivery. It usually resolves without intervention and is not typically a cause for concern.
Choice D rationale:
Transient circumoral cyanosis is often seen in newborns and can occur when the baby is crying or feeding. It usually resolves on its own and is not typically a cause for concern.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
When providing postpartum care teaching to a client, the nurse should include accurate and appropriate information. Option b) "You can expect your breasts to be firm and tender 3 to 5 days after delivery" is a correct statement.
Breast engorgement is a common occurrence around the third to fifth day after delivery as the breasts transition from producing colostrum to mature milk. This can cause the breasts to become firm, swollen, and tender. It is important for the client to be aware of this normal physiological change and to understand how to manage it effectively, such as by applying warm or cold compresses, expressing milk, and ensuring proper breastfeeding techniques.
Option a) "Your bleeding will remain bright red for the next 6 to 8 weeks" is an incorrect statement. After childbirth, the bleeding, called lochia, typically progresses from bright red to a pinkish color and then to a yellowish-white discharge. The duration and characteristics of lochia can vary for each individual, but it generally resolves within a few weeks.
Option c) "You don't need to use birth control if you are exclusively breastfeeding" is an incorrect statement. While breastfeeding can provide some natural contraception, it is not foolproof, and the client can still ovulate and become pregnant. It is important for the client to discuss and choose a suitable method of contraception with her healthcare provider.
Option d) "You should begin performing Kegel exercises 6 to 7 weeks after delivery" is an incorrect statement. Kegel exercises, which strengthen the pelvic floor muscles, can be started as early as the immediate postpartum period and are beneficial for promoting bladder and bowel control, as well as aiding in postpartum recovery. The client can begin performing Kegel exercises soon after delivery, as guided by her healthcare provider.
Correct Answer is D
Explanation
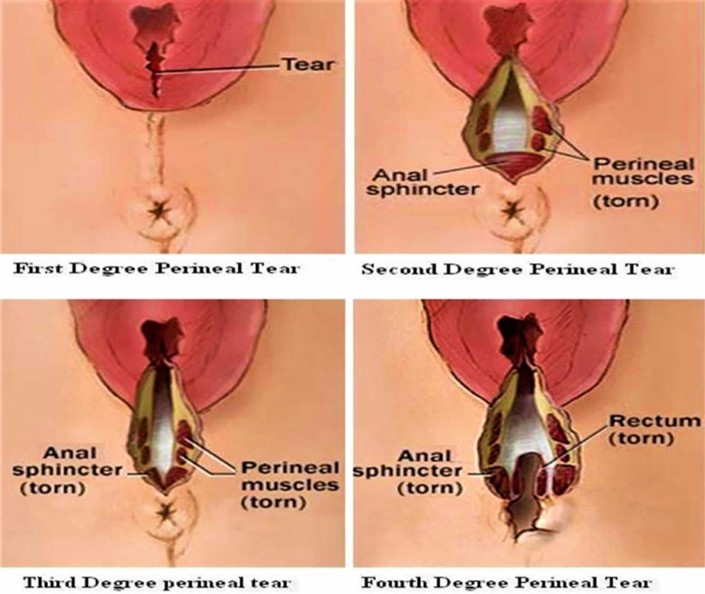
A fourth-degree laceration involves a tear that extends through the perineal muscles and extends to the anal sphincter. This type of laceration requires careful management to promote healing and prevent infection. Applying a moist, warm compress to the perineum helps to promote blood flow, reduce swelling, and provide comfort to the client.
Option a) Providing the client with a cool sitz bath is not appropriate for a fourth-degree laceration. Cool sitz baths are typically used for relieving discomfort and reducing swelling in cases of perineal trauma, but in the case of a fourth-degree laceration, warm compresses are preferred.
Option b) Administering methylergonovine 0.2 mg IM is not necessary for a fourth-degree laceration. Methylergonovine is a medication used to promote uterine contractions and prevent postpartum hemorrhage. However, it is not specifically indicated for the management of perineal lacerations.
Option c) Applying povidone-iodine to the client's perineum after she voids is not recommended for a fourth-degree laceration. Povidone-iodine is an antiseptic solution used to disinfect the skin. However, it is not typically used on open wounds, such as perineal lacerations, as it may delay wound healing.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today