A nurse is caring for a client who is receiving oxytocin for the induction of labor and notes late decelerations of the fetal heart rate on the monitor tracing. The nurse should take which of the following actions?
Administer misoprostol 25 mcg vaginally.
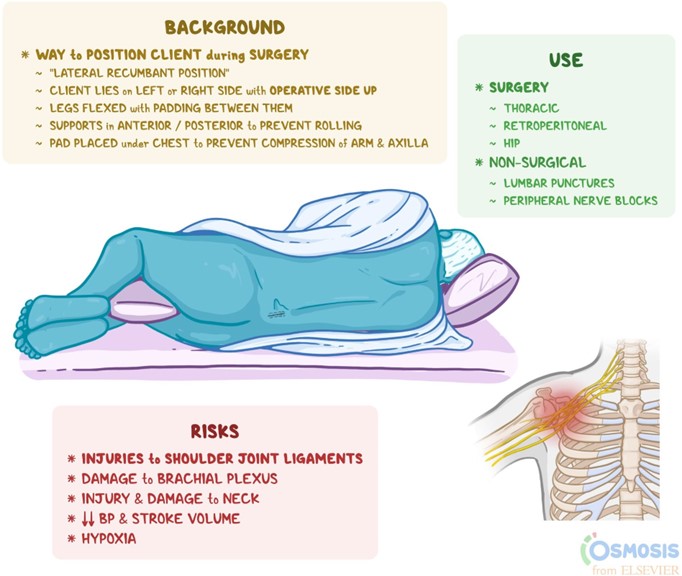
Place the client in a lateral position.
Administer oxygen via a face mask at 2 L/min.
Decrease the maintenance IV solution infusion rate.
The Correct Answer is B
Late decelerations are a type of fetal heart rate (FHR) pattern that indicate fetal hypoxia (lack of oxygen) due to uteroplacental insufficiency (decreased blood flow to the placenta). They are defined as a gradual decrease in FHR that occurs after the peak of a uterine contraction and returns to baseline after the end of the contraction¹. Late decelerations are associated with adverse neonatal outcomes, such as low Apgar scores, acidosis, and neonatal intensive care unit admission².
The nurse should take immediate actions to improve fetal oxygenation and blood flow when late decelerations are detected. The first and most important action is to place the client in a lateral position, either left or right, to reduce compression of the inferior vena cava and increase uterine perfusion. This can improve fetal oxygenation and reduce the severity of late decelerations¹³.
The other actions that the nurse should take are:
- Discontinue oxytocin infusion if it is being used for induction or augmentation of labor, as it can cause uterine tachysystole (excessive contractions) and worsen uteroplacental insufficiency¹³.
- Administer oxygen to the client at 8 to 10 L/min via a nonrebreather face mask to increase maternal oxygen saturation and fetal oxygen delivery¹³.
- Increase intravenous (IV) fluid infusion rate to maintain maternal hydration and blood pressure, which can improve uterine blood flow¹³.
- Notify the provider and prepare for possible operative delivery if late decelerations persist or fetal distress occurs¹³.
- Provide emotional support and reassurance to the client and family, as late decelerations can cause anxiety and fear⁴.
The other options are not actions that the nurse should take:
- a) Administer misoprostol 25 mcg vaginally. This is not correct because misoprostol is a medication that is used to induce labor by ripening the cervix and stimulating contractions. It is not indicated for late decelerations and can cause uterine hyperstimulation and fetal distress⁵.
- c) Administer oxygen via a face mask at 2 L/min. This is not correct because this is too low of an oxygen flow rate to improve fetal oxygenation. The recommended oxygen flow rate for late decelerations is 8 to 10 L/min via a nonrebreather face mask¹³.
- d) Decrease the maintenance IV solution infusion rate. This is not correct because this can cause maternal dehydration and hypotension, which can reduce uterine blood flow and worsen fetal hypoxia. The nurse should increase the IV fluid infusion rate to maintain maternal hydration and blood pressure¹³.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
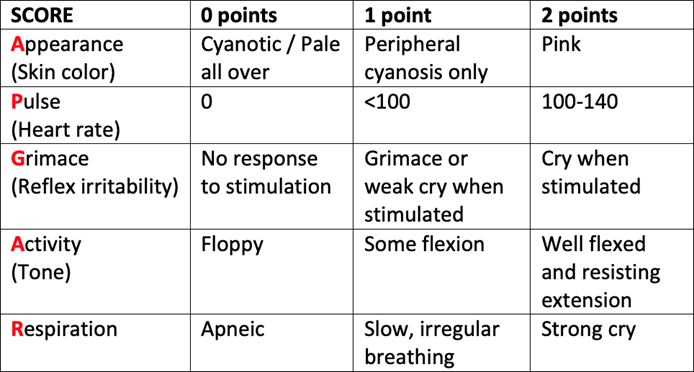
The Apgar score is a method for assessing the health and well-being of a newborn baby immediately after birth. It is based on five criteria: appearance (skin color), pulse (heart rate), grimace (reflex irritability), activity (muscle tone), and respiration (breathing effort). Each criterion is given a score of 0, 1, or 2, depending on the baby's condition. The total score ranges from 0 to 10, with higher scores indicating better health. The Apgar score is determined at one and five minutes after birth, and sometimes at 10 minutes if the score is low or the baby needs resuscitation. The purpose of the Apgar score is to identify babies who need immediate medical attention and to monitor their response to treatment. The Apgar score is not a predictor of long-term outcomes or developmental problems .
One of the criteria that the nurse should measure when assigning an Apgar score is muscle tone. Muscle tone refers to the degree of tension or stiffness in the baby's muscles. It reflects the baby's neuromuscular function and oxygenation. Muscle tone can be assessed by observing the baby's posture, movement, and resistance to passive flexion or extension of the limbs .
The scoring system for muscle tone is as follows:
- Score 0: No movement; limp and floppy
- Score 1: Some flexion of arms and legs; weak or sluggish movement
- Score 2: Active movement; arms and legs flexed and resist extension
Therefore, the newly hired nurse who says that the nurse should measure the newborn's muscle tone
when assigning an Apgar score indicates an understanding of the teaching.
The other statements show a lack of knowledge or misunderstanding of the Apgar scoring:
- a) "The nurse should determine the Apgar score at 2 and 7 minutes after birth." This is not correct because the standard times for determining the Apgar score are one and five minutes after birth, not two and seven minutes. The one-minute score reflects how well the baby tolerated the delivery process, while the five-minute score reflects how well the baby adapted to the extrauterine environment .
- b) "The nurse should identify that the newborn is in severe distress with an Apgar score of 8." This is not correct because an Apgar score of 8 indicates that the newborn is in good condition and does not need any intervention. An Apgar score of 7 to 10 means that the newborn has normal vital signs and reflexes and only needs routine care. An Apgar score of 4 to 6 means that the newborn has moderate distress and may need some assistance with breathing or stimulation. An Apgar score of 0 to 3 means that the newborn has severe distress and needs immediate resuscitation .
- c) "The nurse should wait for the first Apgar score before initiating resuscitation efforts." This is not correct because waiting for the first Apgar score can delay life-saving interventions for a newborn who needs resuscitation. The nurse should initiate resuscitation efforts as soon as possible if the newborn shows any signs of distress, such as apnea, gasping, cyanosis, bradycardia, or poor muscle tone. The nurse should not rely on the Apgar score alone to decide whether to resuscitate or not, but use it as a tool to monitor the baby's response to treatment .
Correct Answer is B
Explanation
This is the finding that the nurse should report to the provider following this medication. Butorphanol is an opioid analgesic that can cause respiratory depression as a serious side effect¹. A normal respiratory rate for an adult is 12 to 20 breaths per minute². A respiratory rate of 10/min is below the normal range and could indicate inadequate ventilation and oxygenation. The nurse should monitor the client's oxygen saturation, administer oxygen if needed, and notify the provider of this finding.
The other options are not correct because they are not signs of adverse effects from butorphanol. Let me
explain why:
a) Urinary Output 1 20 mL in 2 hr
This is a normal urinary output for an adult. A normal urinary output is 0.5 to 1 mL/kg/hr³. Assuming an average weight of 70 kg, this would be 35 to 70 mL/hr, or 70 to 140 mL in 2 hr. Therefore, a urinary output of 120 mL in 2 hr is within the normal range and does not need to be reported.
c) Moderate fetal heart rate variability
This is a reassuring sign of fetal well-being. Fetal heart rate variability is the amount of fluctuation in the fetal heart rate from the baseline. Moderate variability is defined as a fluctuation of 6 to 25 beats per minute (bpm) and indicates that the fetus is responsive and has adequate oxygenation⁴. Moderate variability does not need to be reported.
d) Blood pressure 136/88 mm Hg
This is a slightly elevated blood pressure, but not a sign of an adverse effect from butorphanol. Butorphanol does not cause significant changes in blood pressure¹. A normal blood pressure for an adult is less than 120/80 mm Hg⁵. A blood pressure of 136/88 mm Hg is considered elevated, but not hypertensive. The nurse should monitor the client's blood pressure and check for other signs of preeclampsia, such as proteinuria, headache, or visual changes. However, this finding does not need to be reported immediately.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today