A nurse is assessing a newborn who is 4 hr. old. Which of the following findings should the nurse identify as the priority to report to the provider?
Overlapping of the cranial bones
Small, distended white sebaceous glands on the face
Forward and lateral positioning of the ears
Bluish discoloration of the hands and feet
The Correct Answer is D
In a newborn, bluish discoloration of the hands and feet may indicate a condition called peripheral cyanosis, which suggests poor oxygenation. It is important to report this finding to the healthcare provider promptly, as it may indicate a respiratory or circulatory problem that requires immediate attention.
Option a) Overlapping of the cranial bones is a common finding in newborns due to the molding of the head during delivery. This is not a priority finding to report unless there are other signs of concern, such as abnormal head shape or signs of trauma.
Option b) Small, distended white sebaceous glands on the face are called milia and are a normal finding in newborns. They are not a priority finding to report and typically resolve on their own within a few weeks.
Option c) Forward and lateral positioning of the ears is a normal finding in a newborn and is not a priority to report. The ears may appear folded or positioned differently due to the pressure and positioning in the womb.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
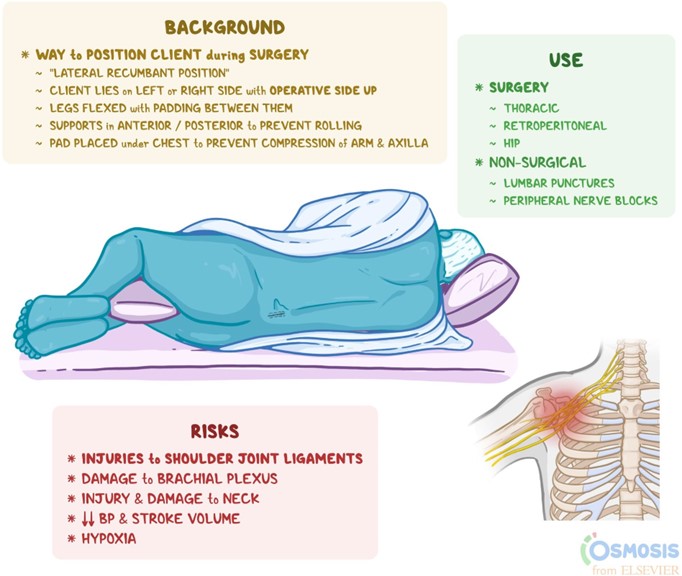
Late decelerations are a type of fetal heart rate (FHR) pattern that indicate fetal hypoxia (lack of oxygen) due to uteroplacental insufficiency (decreased blood flow to the placenta). They are defined as a gradual decrease in FHR that occurs after the peak of a uterine contraction and returns to baseline after the end of the contraction¹. Late decelerations are associated with adverse neonatal outcomes, such as low Apgar scores, acidosis, and neonatal intensive care unit admission².
The nurse should take immediate actions to improve fetal oxygenation and blood flow when late decelerations are detected. The first and most important action is to place the client in a lateral position, either left or right, to reduce compression of the inferior vena cava and increase uterine perfusion. This can improve fetal oxygenation and reduce the severity of late decelerations¹³.
The other actions that the nurse should take are:
- Discontinue oxytocin infusion if it is being used for induction or augmentation of labor, as it can cause uterine tachysystole (excessive contractions) and worsen uteroplacental insufficiency¹³.
- Administer oxygen to the client at 8 to 10 L/min via a nonrebreather face mask to increase maternal oxygen saturation and fetal oxygen delivery¹³.
- Increase intravenous (IV) fluid infusion rate to maintain maternal hydration and blood pressure, which can improve uterine blood flow¹³.
- Notify the provider and prepare for possible operative delivery if late decelerations persist or fetal distress occurs¹³.
- Provide emotional support and reassurance to the client and family, as late decelerations can cause anxiety and fear⁴.
The other options are not actions that the nurse should take:
- a) Administer misoprostol 25 mcg vaginally. This is not correct because misoprostol is a medication that is used to induce labor by ripening the cervix and stimulating contractions. It is not indicated for late decelerations and can cause uterine hyperstimulation and fetal distress⁵.
- c) Administer oxygen via a face mask at 2 L/min. This is not correct because this is too low of an oxygen flow rate to improve fetal oxygenation. The recommended oxygen flow rate for late decelerations is 8 to 10 L/min via a nonrebreather face mask¹³.
- d) Decrease the maintenance IV solution infusion rate. This is not correct because this can cause maternal dehydration and hypotension, which can reduce uterine blood flow and worsen fetal hypoxia. The nurse should increase the IV fluid infusion rate to maintain maternal hydration and blood pressure¹³.
Correct Answer is D
Explanation
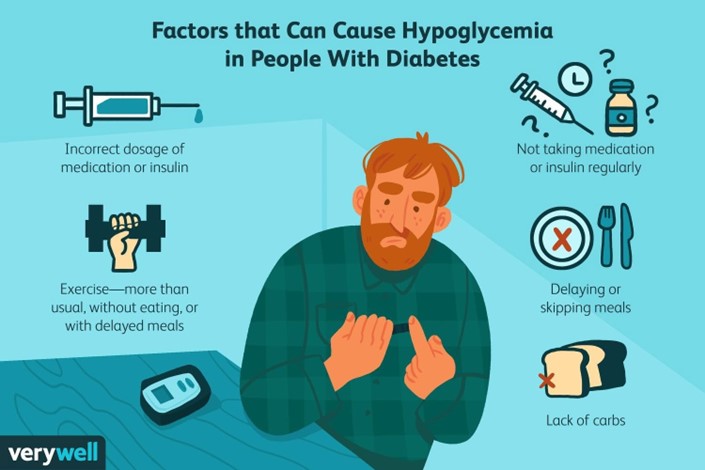
A postpartum client who has type 1 diabetes mellitus and is breastfeeding her newborn should maintain
scheduled mealtimes for herself to prevent hypoglycemia and ensure adequate milk production¹. Breastfeeding may lower glucose levels in the parent and the risk of type 1 and type 2 diabetes in the child¹. Breastfeeding may also help the parent lose weight, prevent diabetes-related complications, and reduce the chances of some cancers¹.
The other options are incorrect because:
a) Taking more insulin with each meal than you did prior to pregnancy may cause hypoglycemia, especially if you are breastfeeding. You should adjust your insulin doses according to your blood glucose levels and carbohydrate intake, and consult your doctor or diabetes educator for guidance²³.
b) Checking your blood glucose levels every 8 hours is not frequent enough to monitor your diabetes during breastfeeding. You should check your blood glucose levels before and after each breastfeeding session, as well as before meals and snacks, at bedtime, and during the night if needed²³.
c) Limiting your carbohydrate intake to 30 grams per day is too restrictive and may impair your milk production and quality, as well as cause hypoglycemia or ketoacidosis. You should consume adequate carbohydrates from healthy sources, such as whole grains, fruits, vegetables, legumes, and dairy products, to meet your energy and nutritional needs²³.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today