A nurse is planning care for a full-term newborn who is receiving phototherapy. Which of the following actions should the nurse include in the plan of care?
Keep the newborn supine throughout treatment.
Dress the newborn in lightweight clothing.
Measure the newborn's temperature every 8 hours.
Avoid using lotion or ointment on the newborn's skin.
The Correct Answer is D
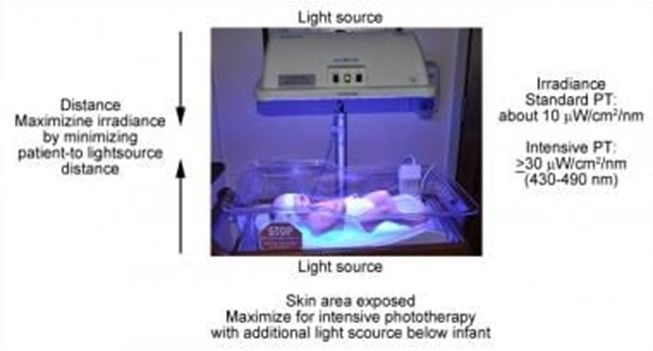
Phototherapy is a treatment that uses light to lower the level of bilirubin in the blood of newborns who have jaundice. Jaundice is a condition that causes yellowing of the skin and eyes due to high levels of bilirubin, a waste product that is normally removed by the liver. Phototherapy helps the body break down and eliminate bilirubin through urine and stool¹.
Phototherapy can be done at home or in the hospital, depending on the severity of jaundice and the type of light used. The most common types of light are fluorescent lamps, halogen lamps, or light-emitting diodes (LEDs). The light can be delivered through overhead units, fiber-optic blankets, or fiber-optic pads. The light should cover as much of the newborn's skin as possible, except for the eyes and genitals¹².
The nurse should follow certain guidelines when caring for a newborn who is receiving phototherapy, such
as:
- Monitor the newborn's temperature, hydration, weight, and urine and stool output regularly
- Protect the newborn's eyes with eye patches or goggles to prevent eye damage
- Turn the newborn every 2 to 4 hours to expose different parts of the body to the light
- Feed the newborn frequently to prevent dehydration and promote bilirubin excretion
- Check the newborn's skin color and bilirubin level periodically to evaluate the effectiveness of
phototherapy
- Provide emotional support and education to the parents about jaundice and phototherapy
One of the important guidelines is to avoid using lotion or ointment on the newborn's skin during phototherapy. This is because lotion or ointment can block the light from reaching the skin and reduce the effectiveness of phototherapy. Lotion or ointment can also cause skin irritation, rash, or burns if they react with the light. The newborn's skin should be clean and dry before phototherapy¹²³.
The other options are not actions that the nurse should include in the plan of care:
- a) Keep the newborn supine throughout treatment. This is not correct because keeping the newborn in one position can limit the exposure of different parts of the body to the light and reduce the effectiveness of phototherapy. The nurse should turn the newborn every 2 to 4 hours to expose different parts of the body to the light¹².
- b) Dress the newborn in lightweight clothing. This is not correct because dressing the newborn in clothing can block the light from reaching the skin and reduce the effectiveness of phototherapy. The newborn should be undressed except for a diaper during phototherapy¹².
- c) Measure the newborn's temperature every 8 hours. This is not correct because measuring the newborn's temperature every 8 hours may not be frequent enough to detect any changes in temperature that may occur during phototherapy. Phototherapy can cause overheating or hypothermia in newborns, depending on the type and intensity of light used. The nurse should monitor the newborn's temperature more often, such as every 2 to 4 hours, and adjust the room temperature or use blankets as needed¹².
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
This is because urine protein of 3+ is a sign of preeclampsia, which is a complication of pregnancy that involves high blood pressure and damage to the kidneys or other organs¹². Preeclampsia can cause serious problems for both the mother and the baby, such as fetal growth restriction, placental abruption, preterm birth, eclampsia, and HELLP syndrome¹². The nurse should report this finding to the provider and monitor the client's blood pressure, reflexes, and fetal well-being. The client may need medication to lower blood pressure and prevent seizures, such as magnesium sulfate or antihypertensives¹².
The other options are not correct because:
a) Deep tendon reflexes of 2+ are normal and do not indicate preeclampsia. Deep tendon reflexes are graded from 0 to 4+, with 2+ being the average response⁶. Increased reflexes (3+ or 4+) may suggest hyperreflexia, which can be a sign of preeclampsia or magnesium toxicity¹⁶.
b) Blood glucose of 110 mg/dL is normal and does not indicate preeclampsia. Blood glucose is the amount of sugar in the blood, and it can vary depending on the time of day, diet, and activity level. The normal range for blood glucose is 70 to 130 mg/dL before meals and less than 180 mg/dL after meals⁷. High blood glucose (hyperglycemia) can be a sign of gestational diabetes, which is a type of diabetes that develops during pregnancy⁷.
d) Hemoglobin of 13 g/dL is normal and does not indicate preeclampsia. Hemoglobin is the protein in red blood cells that carries oxygen throughout the body. The normal range for hemoglobin is 12 to 16 g/dL for women and 14 to 18 g/dL for men⁷. Low hemoglobin (anemia) can be a sign of iron deficiency, bleeding, or infection⁷.
Correct Answer is B
Explanation
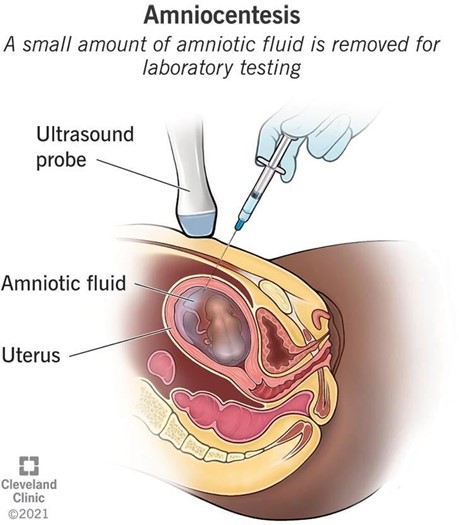
Amniocentesis is a prenatal testing procedure that involves inserting a thin needle through the abdomen into the uterus and withdrawing a small amount of amniotic fluid, which contains fetal cells and other substances¹. The fluid is then analyzed in a laboratory to detect certain chromosomal conditions (such as Down syndrome or trisomy 18), genetic conditions (such as cystic fibrosis or Tay-Sachs disease), or neural tube defects (such as spina bifida or anencephaly) ¹². Amniocentesis can also be used to determine the sex of the fetus, but this is not the primary purpose of the test¹².
The other options are incorrect because:
a) Amniocentesis cannot be scheduled for later today if the client requests it. Amniocentesis requires informed consent, pre-test counseling, and preparation of the equipment and laboratory. Amniocentesis is usually performed between 14 and 20 weeks of gestation, and some medical facilities may perform it as early as 11 weeks, but not on the same day as the request¹²³.
c) The client cannot have an amniocentesis until she is at least 35 years of age. This is a common misconception, as advanced maternal age (35 years or older) is one of the risk factors for chromosomal abnormalities in the fetus, and therefore an indication for amniocentesis. However, amniocentesis can be offered to any pregnant woman who has a personal or family history of genetic conditions, abnormal prenatal screening results, or other indications for fetal diagnosis¹²³.
d) The provider will not schedule a chorionic villus sampling (CVS) to determine the sex of the baby. CVS is another prenatal testing procedure that involves taking a small sample of placental tissue, either through the cervix or the abdomen, and analyzing it for chromosomal or genetic conditions. CVS can also determine the sex of the fetus, but it is usually performed earlier than amniocentesis, between 10 and 13 weeks of gestation. CVS has some advantages over amniocentesis, such as earlier diagnosis and shorter waiting time for results, but it also has some disadvantages, such as higher risk of miscarriage, infection, bleeding, or limb defects¹²⁴. CVS is not routinely offered to all pregnant women, and it is not a substitute for amniocentesis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today