A nurse is caring for a child who has Addison's disease. Which of the following actions should the nurse take?
Place the child on a low-sodium diet
Discuss the manifestations of hyperglycemia with the parents
Monitor the child for fluid volume excess
Teach the parents about cortisol replacement therapy
The Correct Answer is D
Choice A reason: A low-sodium diet is not recommended for a child who has Addison's disease, as they need more sodium to maintain their blood pressure and fluid balance. A high-sodium diet may be advised instead. ¹
Choice B reason: Hyperglycemia, or high blood sugar, is not a common manifestation of Addison's disease, as the condition causes low levels of cortisol, which normally raises blood sugar. Hypoglycemia, or low blood sugar, is more likely to occur and should be monitored and treated. ²
Choice C reason: Fluid volume excess, or edema, is not a common complication of Addison's disease, as the condition causes low levels of aldosterone, which normally retains sodium and water in the body. Fluid volume deficit, or dehydration, is more likely to occur and should be prevented and corrected. ³
Choice D reason: Cortisol replacement therapy is the main treatment for Addison's disease, as it helps restore the normal function of the adrenal glands and prevent adrenal crisis. The parents should be taught about the dosage, timing, and side effects of the medication, as well as the signs and symptoms of underdose and overdose. They should also be instructed to increase the dose during times of stress, illness, or injury, and to carry an emergency injection kit. ⁴.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: The American format for writing dates is month/day/year, so 2/20/2024 is the correct way to write the date February 20, 2024.
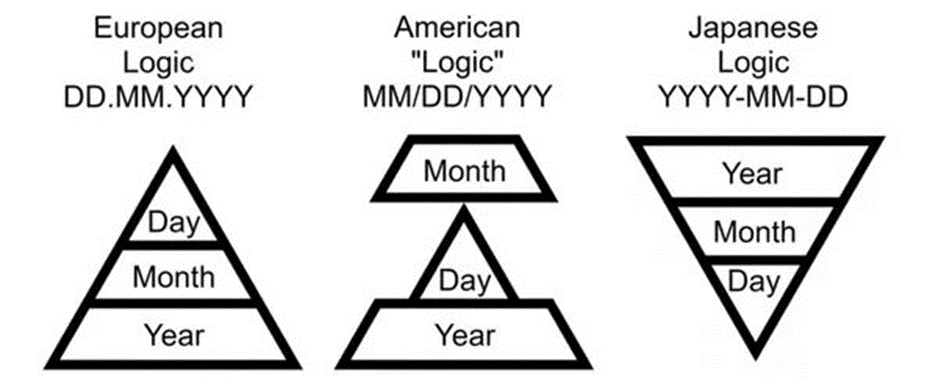
Choice B reason: The European format for writing dates is day/month/year, so 20/2/2024 is not the correct way to write the date in the American format.
Choice C reason: The ISO format for writing dates is year/month/day, so 2024/2/20 is not the correct way to write the date in the American format.
Choice D reason: This is an invalid format for writing dates, as there is no month with 20 days.
Correct Answer is A
Explanation
Choice A reason: Headache is a sign of oxygen toxicity, which is a condition that occurs when the client receives too much oxygen for a prolonged period of time. Oxygen toxicity can damage the lungs and other organs, and cause symptoms such as confusion, seizures, and respiratory failure. The nurse should instruct the client to report headache and adjust the oxygen flow rate accordingly.
Choice B reason: Dry mouth is not a sign of oxygen toxicity, but it could be a side effect of some medications or a result of dehydration. The nurse should instruct the client to drink plenty of fluids and use a humidifier or a nasal saline spray to moisten the mucous membranes.
Choice C reason: Increased appetite is not a sign of oxygen toxicity, but it could be a positive outcome of oxygen therapy, as it indicates improved oxygenation and metabolism. The nurse should encourage the client to eat a balanced diet and monitor their weight and nutritional status.
Choice D reason: Nausea is not a sign of oxygen toxicity, but it could be a side effect of some medications or a symptom of another condition, such as gastroesophageal reflux disease (GERD) or peptic ulcer disease (PUD). The nurse should instruct the client to take their medications as prescribed and avoid foods that trigger nausea, such as spicy, fatty, or acidic foods.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today