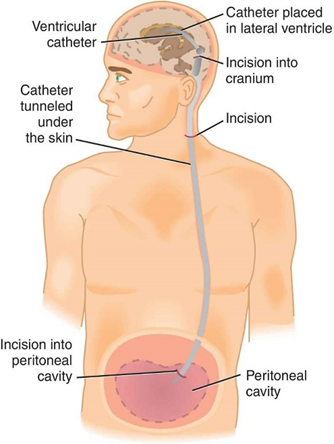
A nurse is caring for a child who is postoperative following the insertion of a ventriculoperitoneal shunt. The nurse should place the child in which of the following positions?
A 45 degree head elevation
On the nonoperative side
Prone
Supine
The Correct Answer is D
A. A 45-degree head elevation: This position can help facilitate venous drainage and reduce intracranial pressure. Elevating the head of the bed may aid in preventing the accumulation of cerebrospinal fluid (CSF) in the brain, which is important after VP shunt insertion to maintain proper drainage. However, this position alone may not be sufficient.
B. On the nonoperative side: Placing the child on the nonoperative side can help reduce pressure on the side where the shunt was inserted, minimizing discomfort and the risk of disruption or displacement of the shunt. However, this position may not directly affect CSF drainage.
C. Prone: Placing the child prone (lying face down) is generally not recommended after VP shunt insertion. This position may increase pressure on the head and interfere with proper CSF drainage, potentially leading to complications.
D. Supine: Placing the child supine (lying on their back) is typically recommended after VP shunt insertion. This position helps promote proper drainage of CSF through the shunt system without placing undue pressure on the surgical site. It also allows for easy monitoring of the child's condition and surgical site.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
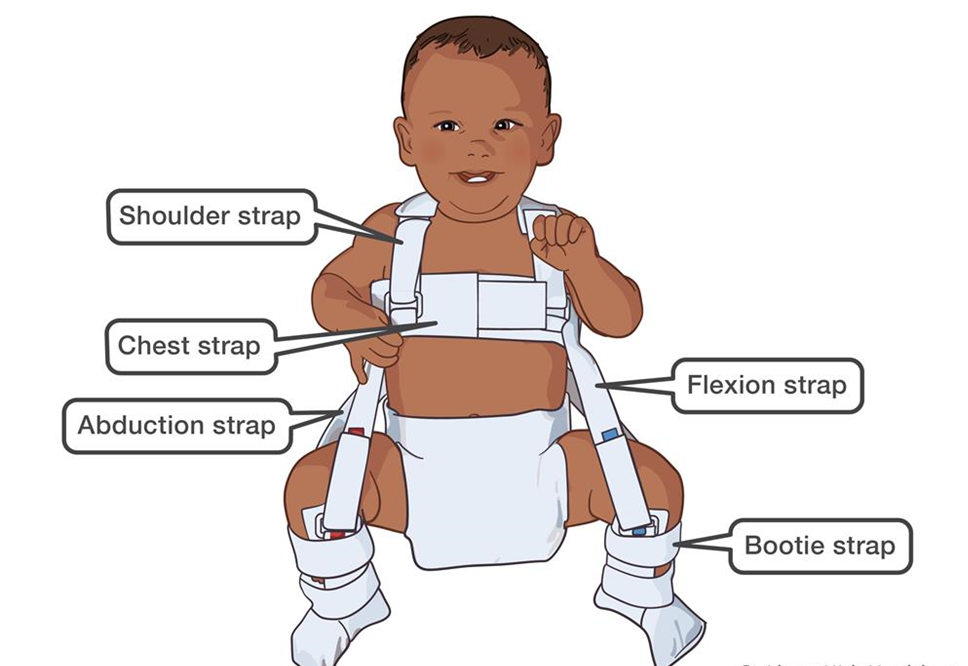
A. "I will use powders & lotion on his skin around the harness clasps."
This statement indicates a misunderstanding. Powders and lotions should generally be avoided around the harness clasps because they can interfere with the proper fit of the harness and cause irritation or discomfort to the baby's skin.
B. “I will remove the harness daily, prior to giving the bath.”
This statement is incorrect. The Pavlik harness is typically not removed for bathing, as it needs to be worn continuously to maintain proper positioning of the hips and promote optimal healing. Removing the harness daily for bathing can disrupt the treatment process and delay progress.
C. "I will adjust the harness straps every day."
This statement indicates a misunderstanding. The harness should not be adjusted daily without guidance from the healthcare provider. The straps of the Pavlik harness are initially adjusted by the healthcare provider to ensure proper fit, and they should remain in place without frequent adjustments to maintain stability and effectiveness.
D. "I will check my baby's skin under the straps frequently."
This statement indicates an understanding of the teaching. It is essential for the mother to regularly check her baby's skin under the harness straps for any signs of irritation, redness, or pressure sores. Monitoring the skin closely allows for early detection of any issues that may arise from wearing the harness.
Correct Answer is B
Explanation
A. Applying suction for 20 seconds:
Suctioning for 20 seconds is within the recommended duration for endotracheal suctioning in children. It allows adequate time for removing secretions without causing excessive trauma to the airway.
B. Introducing the catheter without suction:
This action is incorrect. When performing endotracheal suctioning, the catheter should be introduced into the endotracheal tube while applying suction. Introducing the catheter without suction may not effectively remove secretions and can lead to ineffective suctioning.
C. Rotating the catheter between the thumb and forefinger while suctioning:
Rotating the catheter between the thumb and forefinger while suctioning helps to prevent the catheter from sticking to the airway walls and facilitates the removal of secretions. This action is appropriate and helps ensure effective suctioning.
D. Allowing the child to rest for 30 to 60 seconds between suctioning passes:
Allowing the child to rest between suctioning passes helps minimize hypoxia and discomfort during the procedure. This action is appropriate and ensures that the child has adequate time to recover before the next suctioning pass.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today