A nurse is caring for a client who has preeclampsia and is receiving magnesium sulfate. Which of the following clinical findings should the nurse instruct the client to report?
Increased respiratory rate
Increased fetal movement
Increased urinary output
Increased muscle weakness
The Correct Answer is D
When caring for a client with preeclampsia receiving magnesium sulfate, the nurse should instruct the client to report any increased muscle weakness. Magnesium sulfate is a medication commonly used to prevent and treat seizures in clients with preeclampsia. However, one of the side effects of magnesium sulfate is muscle weakness. If the client experiences an increase in muscle weakness, it could indicate magnesium toxicity, which requires immediate medical attention.
Option a) Increased respiratory rate is not typically associated with magnesium sulfate administration. However, respiratory depression is a potential side effect, so a decreased respiratory rate should be reported.
Option b) Increased fetal movement is generally considered a positive sign of fetal well-being and is not a concern that needs to be reported.
Option c) Increased urinary output is not typically a concerning finding. In fact, maintaining adequate urine output is desired in clients with preeclampsia to ensure proper kidney function. However, a sudden decrease in urinary output or signs of dehydration should be reported.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
This is because a low pulse oximetry reading can indicate that the newborn is hypoxic and needs suctioning of the nasopharynx to clear any secretions that may be obstructing the airway²⁴. Hypoxia can cause bradycardia, acidosis, and brain injury in newborns, and should be corrected as soon as possible². The normal range of pulse oximetry for a newborn is 95% to 100%².
The other options are not correct because:
b) The newborn's respiratory rate is irregular
This is not a sign that suctioning is needed, as it is a normal finding in newborns. Newborns have periodic breathing patterns, which involve alternating periods of rapid and slow breathing, with occasional pauses of up to 10 seconds². This does not indicate respiratory distress or hypoxia, and does not require intervention unless the pauses are longer than 10 seconds or associated with cyanosis or bradycardia².
c) The newborn is beginning to cough
This is not a sign that suctioning is needed, as it is a normal reflex that helps the newborn clear the airway of secretions. Coughing can also stimulate breathing and prevent apnea in newborns². Coughing does not indicate respiratory distress or hypoxia, and does not require intervention unless it is persistent or associated with other signs of respiratory compromise².
d) The newborn's respiratory rate is 32/min
This is not a sign that suctioning is needed, as it is within the normal range for a newborn. The normal respiratory rate for a newborn is 30 to 60 breaths per minute². A respiratory rate that is too high or too low can indicate respiratory distress or hypoxia, and may require suctioning or other interventions².
Correct Answer is A
Explanation
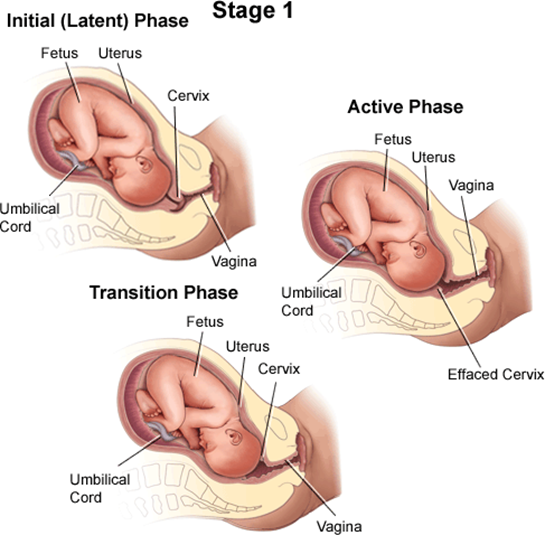
A client who is in labor and reports an urge to have a bowel movement during contractions may be experiencing the transition phase of labor, which is the last and most intense part of the first stage of labor¹². The transition phase occurs when the cervix dilates from 8 to 10 cm and the baby descends into the birth canal¹². The pressure of the baby's head on the rectum can cause a sensation of needing to defecate¹². The transition phase can last from 15 minutes to an hour or more, and it can be accompanied by other signs, such as strong, regular, and painful contractions lasting 60 to 90 seconds; increased bloody show; nausea and vomiting; shaking and shivering; and emotional changes such as irritability, anxiety, or excitement¹²³.
The nurse should reassess the client who reports an urge to have a bowel movement during contractions because this may indicate that the client is close to delivering the baby and needs to be prepared for the second stage of labor, which involves pushing and giving birth¹². The nurse should check the client's cervical dilation, fetal heart rate, and maternal vital signs, and notify the provider if the client is fully dilated or shows signs of fetal or maternal distress¹². The nurse should also support the client's coping strategies, such as breathing techniques, relaxation methods, or pain relief options, and encourage the client not to push until instructed by the provider¹².
b) A sense of excitement and warm, flushed skin are not signs that require reassessment by the nurse. These are normal emotional and physiological responses to labor that reflect increased adrenaline levels and blood flow¹⁴. They do not indicate any complications or imminent delivery.
c) Progressive sacral discomfort during contractions is not a sign that requires reassessment by the nurse. This is a common symptom of labor that results from the pressure of the baby's head on the sacrum and nerves in the lower back¹⁴. It does not indicate any problems or imminent delivery.
d) Intense contractions lasting 45 to 60 seconds are not signs that require reassessment by the nurse. These are typical characteristics of active labor contractions, which occur when the cervix dilates from 4 to 8 cm¹⁴. They do not indicate any complications or imminent delivery.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today