A nurse is caring for a client who is 24 hr postoperative following a cesarean birth.
Select 1 condition and 1 client finding to fill in each blank in the following sentence.
The client is at risk for developing
The Correct Answer is {"dropdown-group-1":"A","dropdown-group-2":"B"}
A. Postpartum hemorrhage is incorrect because the client has scant lochia rubra and a firm fundus at the umbilicus, which indicate normal uterine involution and bleeding.
B. Seizures is correct because the client has signs of severe preeclampsia, such as headache, blurred vision, nausea, hyperreflexia, and clonus. These are indications of increased intracranial pressure and cerebral edema, which can lead to seizures or eclampsia.
C. Hyperglycemia is incorrect because there is no evidence of diabetes mellitus or gestational diabetes in the client's history or findings.
D. Hypoxemia is incorrect because there is no evidence of respiratory distress or impaired gas exchange in the client's history or findings.
E. Infection is incorrect because the client has no signs of infection, such as fever, malaise, foul-smelling lochia, or elevated WBC count.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason
While thinning of secretions can be a positive sign, it's not always visible. A decrease in peak inspiratory pressure is a more objective indicator of improved airway patency.
Choice B reason.
Peak inspiratory pressure is the maximum pressure required to push air into the lungs. If suctioning is effective, it will remove secretions and reduce airway resistance, leading to a decrease in peak inspiratory pressure.
Choice C reason:
While a productive cough can indicate that secretions are being moved, it doesn't directly measure the effectiveness of suctioning.
Choice D reason:
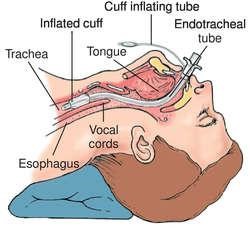
Flattening of the artificial airway cuff: Flattening of the artificial airway cuff is not a relevant indicator of the effectiveness of suctioning. The cuff of an endotracheal tube is inflated to prevent air leaks around the tube and to maintain proper ventilation. It is not directly related to the effectiveness of suctioning.
Correct Answer is C
Explanation
A. Constipation is not a common complication of vacuum-assisted birth. It may be related to other factors such as dehydration, opioid use, or decreased mobility.
B. Urinary urgency is not a common complication of vacuum-assisted birth. It may be related to other factors such as bladder trauma, infection, or diuretic use.
C. Cervical laceration is a common complication of vacuum-assisted birth. It occurs when the vacuum cup causes damage to the cervix during delivery. It can lead to bleeding, infection, or cervical incompetence in future pregnancies.
D. Retained placenta is not a common complication of vacuum-assisted birth. It may be related to other factors such as placenta accreta, uterine atony, or manual removal of the placenta.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today