A nurse is collecting data from a 4-year-old child. Which of the following findings should the nurse expect?
Heart rate 110/min
Capillary refill greater than 3 seconds
Weight gain of 0.9 kg (2 lb) in a year
Respiratory rate 32/min
The Correct Answer is A
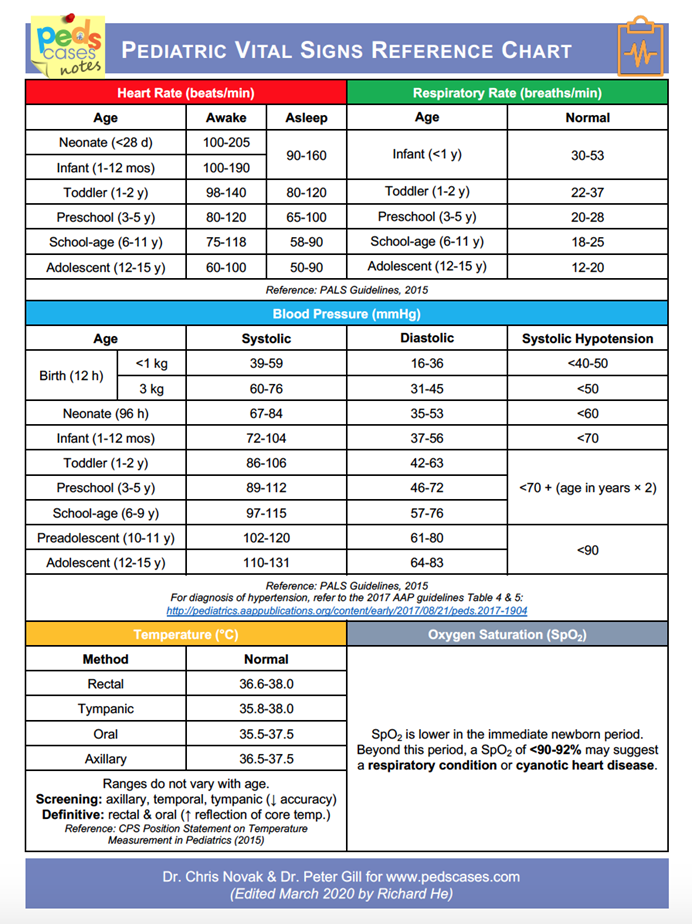
A. Heart rate 110/min: A heart rate of 110 beats per minute is within the normal range for a 4-year-old child. The typical heart rate for this age is between 80 to 120 beats per minute.
B. Capillary refill greater than 3 seconds: Capillary refill time should be less than 2 seconds in a healthy child. A refill time greater than 3 seconds may indicate poor perfusion or dehydration, which is abnormal.
C. Weight gain of 0.9 kg (2 lb) in a year: A weight gain of 2 pounds in a year is below the expected range for a 4-year-old. Children in this age group typically gain around 4-5 pounds per year as they grow.
D. Respiratory rate 32/min: The normal respiratory rate for a 4-year-old child is typically between 20 to 30 breaths per minute. A rate of 32/min is slightly elevated and may indicate respiratory distress or other issues.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. "Bend forward from the waist with your head and arms downward." This position, known as the Adam’s forward bend test, is commonly used to screen for scoliosis. It allows the nurse to observe for any asymmetry in the rib cage or spine, which could indicate scoliosis.
B. "Lie prone on the examination table." Lying prone (face down) does not allow for the assessment of spinal curvature or rib asymmetry. This position is not useful for scoliosis screening.
C. "Touch your chin to your chest, and then look up at the ceiling." These movements assess neck flexibility and range of motion, which are not relevant for screening scoliosis.
D. "Turn to the side, and remain in a relaxed position." Turning to the side and relaxing does not provide the necessary view of the spine to assess for scoliosis. This position does not allow for a clear view of any asymmetry in the spine or ribs.
Correct Answer is ["3.8"]
Explanation
Convert the child’s weight to kg:
22 lb ×1kg/2.2lb = 10 kg
Calculate the daily dose:
1.5 mg/kg/day × 10 kg=15mg/day
Divide the total daily dose by the number of doses per day (every 6 hours):
15mg/day ÷ 4doses/day =3.75mg/dose
Convert the dose to mL using the concentration:
3.75mg × 1 mL/1 mg = 3.75 mL
Round to the nearest tenth:
3.75mL≈ 3.8 mL
Answer: The nurse should administer 3.8 mL per dose.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today