A nurse is contributing to the plan of care for a client who practices Islam. Which of the following questions should the nurse ask the client to clarify the client's religious preferences?
"Do you receive Holy Communion?"
"Do you follow a kosher diet?"
"Do you consume pork products?"
"Do you oppose receiving a blood transfusion if it is needed?”
The Correct Answer is C
The correct answer is Choice C: "Do you consume pork products?"
Choice C rationale: Islamic dietary laws, also known as Halal, prohibit the consumption of pork and its by-products. By asking the client about their consumption of pork products, the nurse demonstrates cultural sensitivity and ensures that the client's dietary preferences and religious practices are respected while under the facility's care.
Choice A rationale: Asking the client if they receive Holy Communion is not appropriate, as this practice is associated with Christianity rather than Islam. This question does not effectively address the client's religious preferences or needs in relation to their Islamic faith.
Choice B rationale: Inquiring about adherence to a kosher diet is not relevant, as this dietary practice is specific to Judaism and does not pertain to the Islamic faith. The nurse should be aware of the distinctions between religious practices when providing culturally competent care.
Choice D rationale: There is no general prohibition against blood transfusions in Islam. Islamic teachings generally permit medical treatments, including blood transfusions, when deemed necessary for the well-being and preservation of life. Asking the client about opposition to blood transfusions would not be the most effective way to clarify their religious preferences in the context of Islam.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
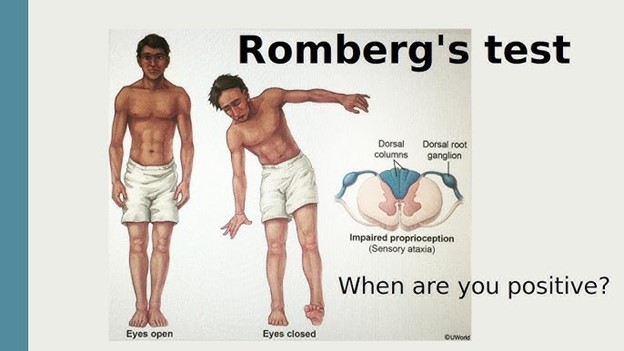
The correct answer is choice A: "Stand with your feet together and your arms at your sides."
Choice A rationale:
This statement is correct. The nurse should instruct the client to stand with their feet together and their arms at their sides for a Romberg test. This position helps to assess the client's ability to maintain balance with minimal sensory input, evaluating their proprioception and vestibular function.
Choice B rationale:
The instruction about the tuning fork is unrelated to the Romberg test. The tuning fork is commonly used to assess hearing and vibratory sensations, not balance.
Choice C rationale:
This statement is unrelated to the Romberg test. Mentioning the lateral side of the foot suggests a neurological examination related to assessing reflexes, such as the Babinski reflex.
Choice D rationale:
This instruction pertains to a different test known as the "finger-to-nose" test, which is used to assess coordination, not balance.
Correct Answer is ["13.6"]
Explanation
The correct answer is 13.6 kg.
To convert pounds to kilograms, the formula is weight in pounds divided by 2.2. Given the child's weight is 30 lb, the calculation would be 30 / 2.2 ≈ 13.64 kg. Rounding to the nearest tenth gives us 13.6 kg.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today