A nurse is performing a neurological assessment for a client who has head trauma. Which of the following assessments will give the nurse information about the function of cranial nerve III?
Ask the client to shrug his shoulders against passive resistance
Instruct the client to look up and down without moving his head
Observe the client's ability to smile and frown
Have the client stand with his eyes closed and touch his nose
The Correct Answer is B
Choice A: Ask the client to shrug his shoulders against passive resistance is not an assessment that will give the nurse information about the function of cranial nerve III. This assessment will test the function of cranial nerve XI, which is the accessory nerve. The accessory nerve innervates the trapezius and sternocleidomastoid muscles, which are involved in shoulder and neck movements.
Choice B: Instruct the client to look up and down without moving his head is an assessment that will give the nurse information about the function of cranial nerve III. Cranial nerve III is the oculomotor nerve, which innervates four of the six extraocular muscles that control eye movements. The oculomotor nerve also controls pupil size and lens shape. By instructing the client to look up and down without moving his head, the nurse can assess the ability of the oculomotor nerve to move the eyes vertically and adjust to different distances.
Choice C: Observe the client's ability to smile and frown is not an assessment that will give the nurse information about the function of cranial nerve III. This assessment will test the function of cranial nerve VII, which is the facial nerve. The facial nerve innervates the muscles of facial expression, which are involved in smiling, frowning, blinking, and other facial movements.
Choice D: Have the client stand with his eyes closed and touch his nose is not an assessment that will give the nurse information about the function of cranial nerve III. This assessment will test the function of cranial nerve VIII, which is the vestibulocochlear nerve. The vestibulocochlear nerve innervates the inner ear and is responsible for hearing and balance. By having the client stand with his eyes closed and touch his nose, the nurse can assess the ability of the vestibulocochlear nerve to maintain equilibrium and coordination.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because this client has signs of brain death, such as severe head injuries, low respiratory rate, and unresponsiveness. The nurse should tag this client as black, which means deceased or expectant.
Choice B Reason: This is incorrect because this client has non-life-threatening injuries, such as a simple fracture and scratches. The nurse should tag this client as green, which means minor or delayed care.
Choice C Reason: This is incorrect because this client has minor injuries and is able to walk around. The nurse should tag this client as green, which means minor or delayed care.
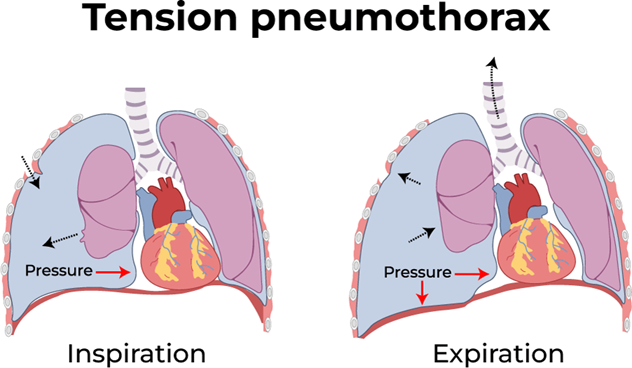
Choice D Reason: This is correct because this client has a life-threatening condition called tension pneumothorax, which requires immediate care. This client has a life-threatening condition called tension pneumothorax, which is caused by air leaking into the pleural space and compressing the lung and the heart. This can lead to respiratory failure, cardiac arrest, and death if not treated immediately. The hissing sound indicates that air is escaping from the lung through the wound. The nurse should tag this client as red, which means immediate care is needed.
Correct Answer is A
Explanation
Choice A Reason: This is correct. The nurse should remove both of the elastic bandages from the leg, as they can impair blood flow and increase tissue damage. The nurse should also elevate the leg and keep it immobile to reduce venom absorption.
Choice B Reason: This is incorrect. The nurse should not discharge the client, as they may develop serious complications from the snake bite, such as swelling, bleeding, infection, or shock. The client should be monitored closely and treated accordingly.
Choice C Reason: This is incorrect. The nurse should not obtain a prescription for the appropriate anti-venom, as this is not within their scope of practice. The nurse should notify the physician and provide supportive care until the physician arrives and decides whether to administer anti-venom or not.
Choice D Reason: This is incorrect. The nurse should not obtain a prescription for pain medication, as this may mask the symptoms of venom toxicity or cause adverse reactions with anti-venom. The nurse should use non- pharmacological methods to relieve pain, such as ice packs or distraction.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today