A nurse is planning care for a client who is postoperative following insertion of an arteriovenous graft in their left forearm. Which of the following actions should the nurse include in the plan of care?
Check the pulse distal to the graft.
Splint the left forearm to prevent damage to the graft.
Collect blood specimens from the graft.
Keep the left forearm below the level of the heart.
The Correct Answer is A
A Checking the pulse distal (beyond) to the AV graft site is crucial to assess peripheral circulation. It helps determine if the graft is adequately perfusing blood to the distal extremity. Absence or weak pulse distal to the graft could indicate graft malfunction or complications such as thrombosis or inadequate blood flow.
B. Splinting the forearm may help immobilize the arm and reduce movement that could potentially disrupt the AV graft site. However, immobilization should be balanced with promoting mobility and preventing complications such as joint stiffness or pressure injuries.
C. Drawing blood from the AV graft could introduce infection risk or damage the graft site. It is standard practice to avoid using the AV graft for routine blood draws
D. Positioning the forearm below the level of the heart promotes venous return and reduces swelling or edema in the extremity. However, for an AV graft, maintaining the arm in a dependent position should be avoided to prevent excessive pressure on the graft site or compromising blood flow.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is {"dropdown-group-1":"B","dropdown-group-2":"C"}
Explanation
The nurse should plan to first administer 0.9% sodium chloride followed by Insulin
Rationale
Intravenous fluid resuscitation takes priority in the management of DKA due to the severe dehydration that occurs due to osmotic diuresis.
The next step is to administer intravenous insulin infusion as per the prescribed rate.
Correct Answer is D,B,A,C
Explanation
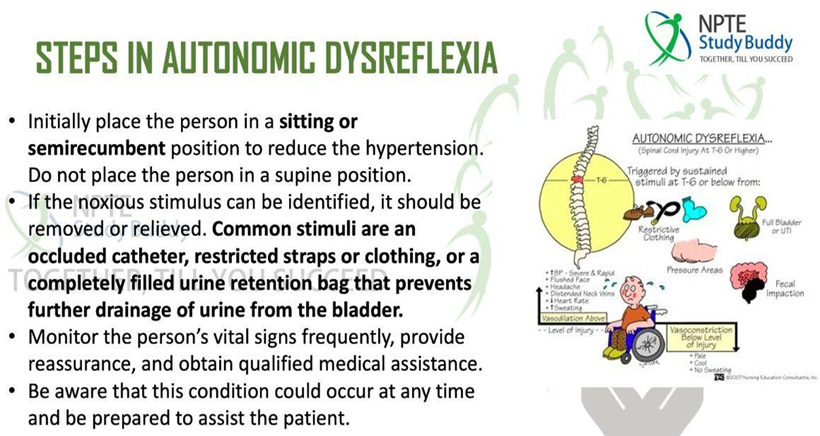
Step D (Place the client in an upright sitting position): Elevating the client's head and upper body to an upright position helps to reduce blood pressure by promoting venous pooling in the lower extremities.
Step B (Confirm that the client's bladder is empty): Autonomic dysreflexia is often triggered by bladder distention or urinary retention. By confirming and addressing urinary issues promptly, the nurse can remove the triggering stimulus.
Step A (Administer an antihypertensive medication intravenously): In severe cases where blood pressure remains dangerously high despite other interventions, such as positioning and addressing bladder issues, antihypertensive medications may be necessary to lower blood pressure quickly and prevent complications.
Step C (Indicate the risk for autonomic dysreflexia in the client's medical record): Documentation of the occurrence of autonomic dysreflexia, its triggers, and interventions used is essential for continuity of care. It informs other healthcare providers about the client's condition and helps in implementing preventive strategies.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today