A nurse is preparing to administer a medication to a client for the first time. Which of the following actions should the nurse take to help ensure safe medication administration?
Read the medication label twice prior to administration.
Use one patient identifier prior to medication administration.
Access the online drug formulary for an unfamiliar medication.
Ask the client if they have ever taken a similar medication.
The Correct Answer is A
A. Read the medication label twice prior to administration.
This action is crucial to ensure that the nurse correctly identifies the medication and verifies the dosage before administering it to the patient. By double-checking the medication label, the nurse can confirm that they have the right medication, in the correct dose, for the correct patient, and via the correct route. This practice helps prevent medication errors and promotes patient safety.
B. Use one patient identifier prior to medication administration.
Explanation: Using at least one patient identifier, such as the patient's name or date of birth, is a standard safety practice to confirm the patient's identity before administering any medication. This helps ensure that the medication is given to the right patient, reducing the risk of administering medications to the wrong individual.
C. Access the online drug formulary for an unfamiliar medication.
Explanation: While it's essential to be knowledgeable about medications, relying solely on an online drug formulary for unfamiliar medications may not be sufficient for safe administration. Online resources can provide valuable information, but they should supplement, not replace, comprehensive education and understanding of medications. Nurses should have a solid understanding of the medications they administer and consult additional resources as needed.
D. Ask the client if they have ever taken a similar medication.
Explanation: While it's important to gather information from the patient about their medical history and previous experiences with medications, solely relying on the patient's response may not be sufficient for ensuring safe medication administration. Patients may not always accurately recall or provide complete information about their medication history. Nurses should verify medication orders through appropriate channels and rely on documented medical records whenever possible to confirm medication history and suitability for administration.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
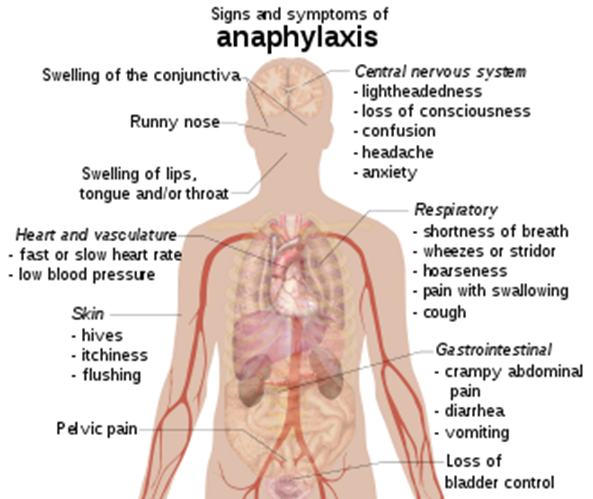
A. A feeling of swelling in the feet: Swelling in the feet can be caused by various factors such as fluid retention, circulatory issues, or certain medical conditions like venous insufficiency. It is not a typical symptom of anaphylaxis, which usually involves more generalized symptoms such as hives, itching, swelling of the face or throat, difficulty breathing, and a drop in blood pressure.
B. Pain at the injection site: Pain at the injection site is a common side effect of receiving an injection or medication. It occurs due to tissue irritation or trauma from the needle. While allergic reactions can cause localized redness, swelling, or itching at the injection site, severe pain alone is not a hallmark symptom of anaphylaxis.
C. A sudden decrease in heart rate: Anaphylaxis typically leads to an increase in heart rate (tachycardia) rather than a decrease. This increase in heart rate is a response to the body's attempt to compensate for the drop in blood pressure caused by anaphylaxis. Bradycardia (a decrease in heart rate) is not a typical feature of anaphylaxis unless it occurs very late in a severe reaction due to profound circulatory collapse.
D. A sharp decrease in blood pressure: This choice is indicative of an understanding of possible anaphylaxis. Anaphylaxis can cause a rapid and severe drop in blood pressure, known as hypotension. This drop in blood pressure is often a key feature of anaphylaxis and can lead to symptoms such as dizziness, fainting, confusion, and shock.
Correct Answer is D
Explanation
A. Extend the client's neck while securing the ties: This action can compromise the client's airway and is not recommended during tracheostomy tie changes. The client's neck should be in a comfortable, neutral position during the procedure.
B. Use a quick-release knot to secure the ties: Quick-release knots are not typically used for securing tracheostomy ties. Instead, a secure knot that can be easily tied and untied is preferred to ensure the stability of the tracheostomy tube.
C. Allow space for three fingers under the ties when securing.
Allowing space for three fingers is not a standard practice for tracheostomy ties. The ties should be snug but not overly tight, typically allowing for one or two fingers’ width to ensure proper fit and comfort.
D. When changing tracheostomy ties, it is essential to maintain airway security and prevent accidental dislodgement of the tracheostomy tube. The nurse should secure the new ties first before removing the old ones to ensure the tracheostomy remains stable.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today