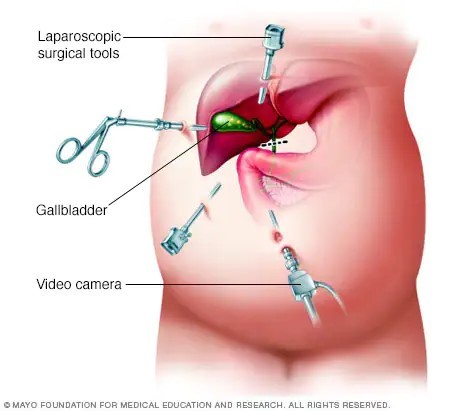
A nurse is reinforcing teaching with a client who is postoperative following a laparoscopic cholecystectomy. Which of the following statements by the client indicates an understanding of the teaching?
“I should eat a high-fat diet for several weeks."
"I should expect to have diarrhea until my diet changes."
"I should expect to have nausea for several days."
"I should leave my steri-strips on until they fall off."
The Correct Answer is D
After a laparoscopic cholecystectomy, steri-strips or adhesive strips are commonly placed over the small incisions. The client should keep the steri-strips in place until they fall off on their own or until they are removed by the healthcare provider during a follow-up visit. Removing the steri-strips prematurely can increase the risk of infection or disrupt the healing process.
"I should eat a high-fat diet for several weeks": After a laparoscopic cholecystectomy, it is important for the client to follow a low-fat diet initially to allow the body time to adjust to the absence of the gallbladder. High-fat foods can be more difficult to digest and may cause digestive discomfort. Gradually introducing small amounts of fat back into the diet is recommended, but a high-fat diet is not appropriate.
"I should expect to have diarrhea until my diet changes": While changes in bowel movements can occur after a cholecystectomy, such as looser stools or changes in frequency, persistent diarrhea is not expected or normal. If the client experiences persistent diarrhea, they should contact their healthcare provider for further evaluation.
"I should expect to have nausea for several days": While some clients may experience mild nausea or discomfort after the surgery, it should generally improve within a few days. If the client experiences persistent or severe nausea, they should contact their healthcare provider.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
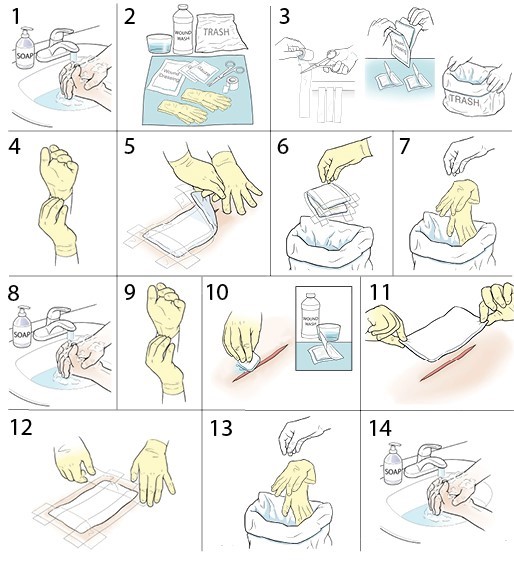
When removing the dressing and cleaning the wound, it is important to start from the center of the wound and work towards the outer edges. This technique helps prevent contamination of the wound by minimizing the risk of dragging bacteria or debris from the surrounding skin into the wound.
The other options listed are not recommended for this specific procedure:
When removing the tape, it is generally recommended to pull it parallel to the skin surface rather than pulling from the center of the dressing. This technique reduces the risk of causing trauma or disrupting the wound.
While it is important to maintain aseptic technique during dressing changes, wearing sterile gloves is not necessary for a wet-to-dry dressing change. Clean, non-sterile gloves are typically sufficient for this procedure, as the dressing material itself is not sterile.
In a wet-to-dry dressing change, the dressing is typically applied moist and allowed to dry over time. Therefore, moistening the dressing before removal is not necessary. The primary goal is to remove the dry dressing, which may adhere to the wound bed, and then clean the wound before applying a fresh dressing.
Correct Answer is D
Explanation
Furosemide works by promoting diuresis, which helps to reduce fluid volume overload in heart failure. Increased urinary output indicates that the medication is effectively removing excess fluid from the body. This can help alleviate symptoms such as edema and fluid retention commonly associated with heart failure. Therefore, an increased urinary output is a positive response to furosemide therapy in this context.
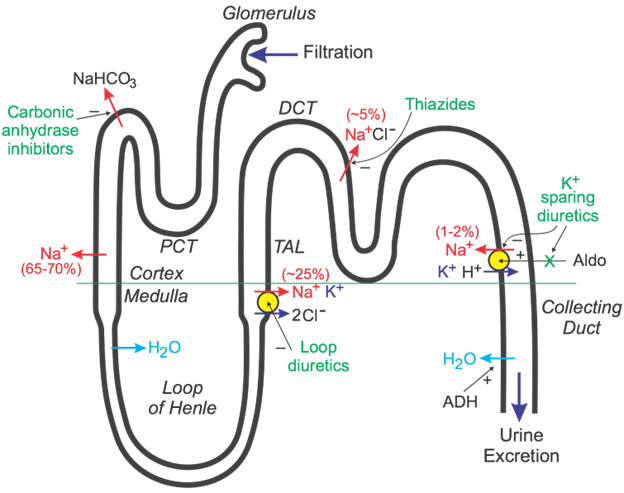
Decreased BUN (blood urea nitrogen) levels and weight loss are also expected outcomes of diuretic therapy, further indicating the effectiveness of the medication. However, a decreased hemoglobin level is not directly related to the efficacy of furosemide and might be indicative of other factors such as anemia or bleeding, requiring further assessment and intervention.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today