A nurse is reviewing the guidelines for documenting client care. Which of the following actions should the nurse plan to take?
Avoid quoting client comments when documenting.
Document giving a dose of pain medication just prior to administration.
Limit documentation to subjective information.
Document information telephoned in by a nurse who left the unit for the day.
The Correct Answer is A
Quoting client comments verbatim in the documentation should be avoided. Instead, the nurse should summarize or paraphrase the relevant information provided by the client. This helps to maintain confidentiality and professionalism in the documentation process.
Documenting giving a dose of pain medication just prior to administration: Documentation should accurately reflect the timing and administration of medications. It is not appropriate to document giving a dose of medication just prior to administering it, as it would not provide an accurate account of the client's care. The medication administration should be documented after it has been given.
Limiting documentation to subjective information: Documentation should include both objective and subjective information. Objective information refers to measurable and observable data, while subjective information represents the client's thoughts, feelings, and experiences.
Including both types of information provides a comprehensive view of the client's condition and the care provided.
Documenting information telephoned in by a nurse who left the unit for the day: Documentation should only include information that has been directly observed or obtained by the nurse providing care. It is not appropriate to document information telephoned in by a nurse who is not present and available to verify or provide additional details. Each nurse should be responsible for documenting their own observations and actions.
Accurate and comprehensive documentation is crucial for maintaining continuity of care, ensuring effective communication among the healthcare team, and promoting the client's safety and well-being. Nurses should adhere to institutional policies and guidelines regarding documentation practices and prioritize accuracy, confidentiality, and professionalism in their documentation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
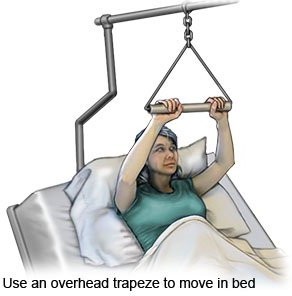
Using the overbed trapeze helps the client strengthen their upper body and improve mobility by allowing them to independently move and reposition themselves in bed. This promotes independence in activities of daily living and reduces reliance on nursing assistance.
Cautioning the client to avoid a prone position while in bed is important for preventing pressure ulcers and maintaining proper positioning, but it does not specifically promote independence and mobility.
Keeping a loose, absorbent dressing over the surgical site is important for wound care and infection prevention, but it does not directly promote mobility or independence.
Maintaining abduction of the client's residual limb with a pillow is important to prevent contractures, but it does not directly promote mobility or independence.
Correct Answer is ["A","C"]
Explanation
A. Assign the client to a negative-pressure airflow room:Varicella zoster (chickenpox) is highly contagious and can be transmitted through airborne droplets.A negative-pressure airflow room helps prevent the spread of the virus to other patients and healthcare workers.
B.Have visitors remain at least 0.91 m (3 feet) away from the client: While maintaining distance is generally advisable, it is not the primary intervention for varicella. The focus should be on preventing transmission through other means.
C.Initiate contact precautions for the client:Correct!Contact precautions are essential for varicella-zoster patients. This includes using gloves and gowns when in direct contact with the client or their environment. Airborne precautions are also recommended because varicella is highly contagious.
D.Administer aspirin if the client develops a fever: Aspirin is generally avoided in children with varicella due to the risk of Reye’s syndrome. Acetaminophen (paracetamol) is a safer choice for fever management.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today