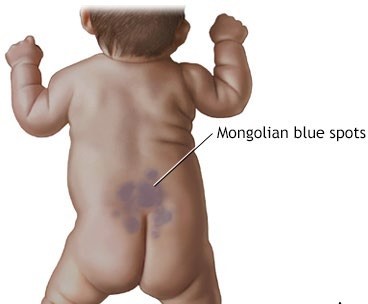
During a physical assessment of a newborn, the nurse observes bluish markings across the newborn's lower back. The nurse interprets this finding as:
Select one:
Milia.
Dermal melanosis.
Stork bites.
Birth trauma.
The Correct Answer is B
Choice A Reason: Milia. This is an incorrect answer that describes a different skin condition. Milia are tiny white or yellow cysts that appear on the nose, chin, or cheeks of newborns. They are caused by the retention of keratin in the sebaceous glands or hair follicles. They usually disappear within a few weeks without treatment.
Choice B Reason: Dermal melanosis. This is a correct answer that explains the finding of bluish markings across the newborn's lower back. Dermal melanosis. This is because dermal melanosis, also known as Mongolian spots, is a common benign skin condition that affects newborns of Asian, African, or Hispanic descent. It is characterized by bluish-gray or brown patches of pigmentation on the lower back, butocks, or extremities. It is caused by the migration of melanocytes from the neural crest to the dermis during embryonic development. It usually fades by 2 to 4 years of age.
Choice C Reason: Stork bites. This is an incorrect answer that refers to another skin condition. Stork bites, also known as salmon patches or nevus simplex, are flat pink or red marks that appear on the forehead, eyelids, nose, upper lip, or nape of the neck of newborns. They are caused by dilated capillaries in the superficial dermis. They usually fade by 18 months of age.
Choice D Reason: Birth trauma. This is an incorrect answer that implies an injury or damage to the newborn's skin or tissues during labor and delivery. Birth trauma can cause bruises, abrasions, lacerations, fractures, or nerve injuries. It is not related to bluish markings on the lower back.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: "You would have seen more symptoms if you had been looking more closely at your baby." This is an inappropriate response that blames the parents for missing the signs of sepsis and does not explain the Reason for the subtle symptoms.
Choice B Reason: "A newborn's immune system isn't mature, so symptoms are subtle and can be hard to recognize." This is an appropriate response that educates the parents about the immunological basis of sepsis in newborns and reassures them that they are not at fault for not noticing the symptoms.
Choice C Reason: "A high fever will always be present in sick newborns, including your baby." This is an incorrect response that contradicts the fact that newborns may not develop fever in response to infection due to their immature immune systems.
Choice D Reason: "A mother's immunity usually protects the infant from illness, but not in this case." This is an inaccurate response that implies that the mother failed to provide adequate immunity to her baby and does not address the question of why the baby did not seem very ill.
Correct Answer is B
Explanation
Choice A Reason: Prepare for IV dextrose administration. This is an incorrect answer that indicates an unnecessary and invasive intervention for an IDM with normal blood glucose. IV dextrose administration is indicated for an IDM with severe or persistent hypoglycemia, which is defined as a blood glucose below 40 mg/dL or below 60 mg/dL after two feedings.
Choice B Reason: Provide routine care, per hospital IDM protocol. This is because a blood glucose of 60 is within the normal range for an IDM, which is 40 to 80 mg/dL. An IDM is a newborn whose mother has pre-existing or gestational diabetes, which can affect the fetal and neonatal glucose metabolism and regulation. An IDM may have hypoglycemia (low blood glucose), hyperglycemia (high blood glucose), or other complications such as macrosomia, polycythemia, or congenital anomalies. An IDM requires routine care and monitoring according to the hospital IDM protocol, which may include blood glucose testing, feeding, temperature regulation, and observation for signs of distress.
Choice C Reason: Place the infant in a warmed incubator. This is an incorrect answer that suggests an irrelevant and potentially harmful action for an IDM with normal blood glucose. Placing the infant in a warmed incubator is indicated for an IDM with hypothermia, which is a low body temperature that can impair glucose utilization and increase oxygen consumption. However, placing the infant in a warmed incubator without proper indication can cause hyperthermia, which is a high body temperature that can lead to dehydration, electrolyte imbalance, or brain damage.
Choice D Reason: Alert the clinician immediately for orders. This is an incorrect answer that implies an urgent and unwarranted situation for an IDM with normal blood glucose. Alerting the clinician immediately for orders is indicated for an IDM with signs of distress or complications, such as apnea, cyanosis, seizures, or jaundice.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today