The Mother-Baby nurse is caring for a two hour old newborn who is 36 4/7 weeks gestation. The nurse assesses that the newborn is experiencing tremors (jiteriness). What nursing action has the highest priority?
Select one:
Obtain a bilirubin level.
Place a pulse oximeter on the newborn.
Obtain a blood glucose level.
Take the newborn's vital signs.
The Correct Answer is C
Choice A Reason: Obtain a bilirubin level. This is an incorrect answer that indicates an irrelevant and unnecessary nursing action for a newborn with tremors or jiteriness. Obtaining a bilirubin level is a nursing action that is indicated for a newborn with jaundice (yellowish discoloration of the skin and mucous membranes), which can occur due to increased bilirubin production or decreased bilirubin excretion. Jaundice does not cause tremors or jiteriness in newborns.
Choice B Reason: Place a pulse oximeter on the newborn. This is an incorrect answer that suggests an inappropriate and insufficient nursing action for a newborn with tremors or jiteriness. Placing a pulse oximeter on the newborn is a nursing action that measures oxygen saturation and heart rate, which can indicate hypoxia (low oxygen level) or distress in newborns. Hypoxia can cause tremors or jiteriness in newborns, but it is not the only or most likely cause. Placing a pulse oximeter on the newborn does not provide enough information to diagnose or treat hypoglycemia.
Choice C Reason: Obtain a blood glucose level. This is because tremors or jiteriness are common signs of hypoglycemia (low blood glucose) in newborns, which can occur due to various factors such as prematurity, maternal diabetes, infection, or cold stress. Hypoglycemia can cause neurological damage or death if not treated promptly and effectively. Obtaining a blood glucose level is a nursing action that has the highest priority for a newborn with tremors or jiteriness, as it can confirm the diagnosis and guide the treatment.
Choice D Reason: Take the newborn's vital signs. This is an incorrect answer that implies an inadequate and delayed nursing action for a newborn with tremors or jiteriness. Taking the newborn's vital signs is a nursing action that monitors temperature, pulse, respiration, and blood pressure, which can indicate general health status and stability in newborns. Taking the newborn's vital signs may reveal signs of hypoglycemia, such as hypothermia, tachycardia, tachypnea, or hypotension, but it is not a specific or definitive test for hypoglycemia. Taking the newborn's vital signs may also waste valuable time that could be used to obtain a blood glucose level and initiate treatment.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
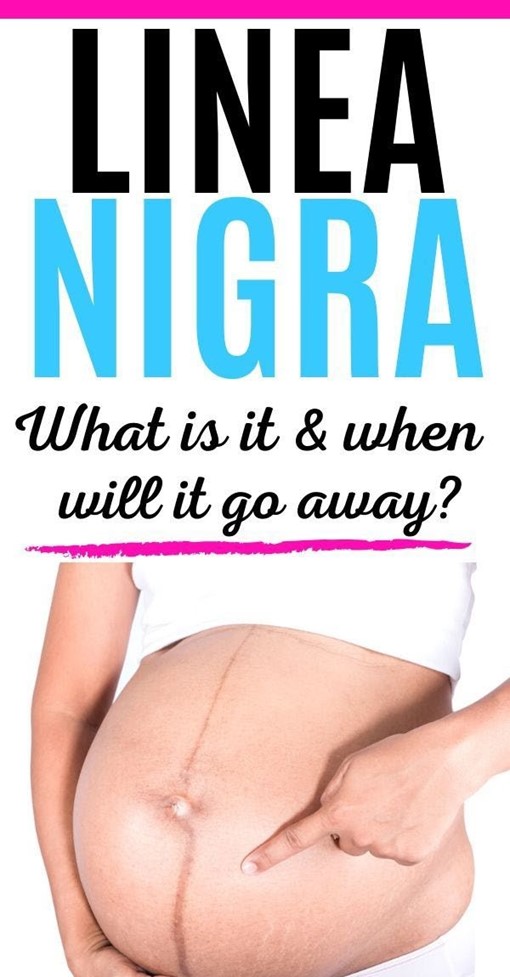
Choice A Reason: Vascular spider veins. This is an incorrect answer that refers to a different skin change that occurs during pregnancy, which affects the blood vessels, not the pigment. Vascular spider veins are small red or purple clusters of blood vessels that appear on the skin, especially on the face, neck, chest, or legs. Vascular spider veins are caused by increased blood volume and hormonal changes, which dilate and rupture the capillaries. Vascular spider veins are harmless and usually disappear after delivery.
Choice B Reason: Linea nigra. This is because linea nigra is a term that refers to a darkened vertical line that appears on the abdomen during pregnancy, which runs from the umbilicus to the pubis. Linea nigra is caused by increased production of melanin, which is a pigment that gives color to the skin and hair. Linea nigra is more common and noticeable in women with darker skin tones, and it usually fades after delivery.
Choice C Reason: Melasma. This is an incorrect answer that refers to a different skin change that occurs during pregnancy, which affects the pigment, but not in a linear patern. Melasma is a term that refers to patches of brown or gray-brown discoloration that appear on the face, especially on the forehead, cheeks, nose, or upper lip. Melasma is also caused by increased production of melanin, but it is influenced by sun exposure and genetic factors. Melasma is also known as chloasma or the mask of pregnancy, and it may persist after delivery.
Choice D Reason: Striae gravidarum. This is an incorrect answer that refers to a different skin change that occurs during pregnancy, which affects the connective tissue, not the pigment. Striae gravidarum are stretch marks that appear on the skin, especially on the abdomen, breasts, hips, or thighs. Striae gravidarum are caused by rapid growth and stretching of the skin, which damage the collagen and elastin fibers. Striae gravidarum are initially red or purple, but they fade to white or silver after delivery.
Correct Answer is B
Explanation
Choice A Reason: Physiologic anemia due to maternal increased plasma volume. This is an incorrect answer that refers to a different condition that affects hemoglobin levels, not blood pressure. Physiologic anemia is a condition where the maternal plasma volume increases more than the red blood cell mass during pregnancy, which dilutes the hemoglobin concentration and lowers the hematocrit value. Physiologic anemia does not cause significant symptoms or complications in pregnant women, as it is an adaptive mechanism that enhances oxygen delivery and prevents fluid overload.
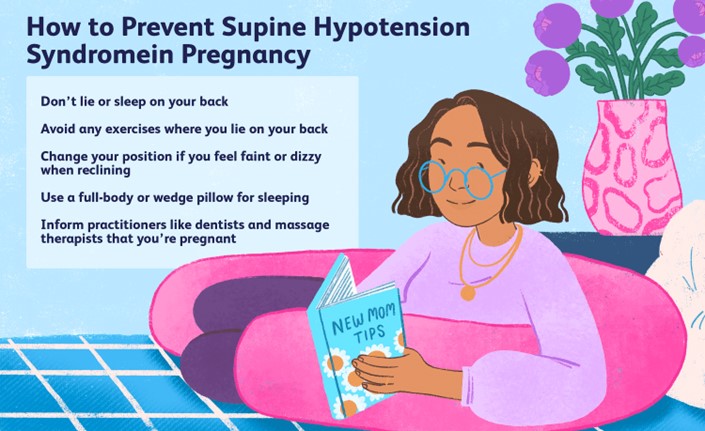
Choice B Reason: Pressure of the gravid uterus on the maternal inferior vena cava and aorta. This is because this statement explains the cause of supine hypotensive syndrome, which is a condition where lying flat on the back causes compression of the major blood vessels by the gravid uterus, which reduces venous return and cardiac output, which lowers blood pressure and perfusion to vital organs. Supine hypotensive syndrome can cause symptoms such as dizziness, lightheadedness, nausea, pallor, or syncope in pregnant women, especially in the third trimester.
Choice C Reason: Pressure of the presenting fetal part on the maternal diaphragm. This is an incorrect answer that indicates a different condition that affects respiratory function, not blood pressure. Pressure of the presenting fetal part on the maternal diaphragm is a result of cephalic engagement or lightening, which occurs when the fetal head descends into the pelvis and occupies more space in the abdominal cavity. Pressure of the presenting fetal part on the maternal diaphragm can cause symptoms such as dyspnea, heartburn, or rib pain in pregnant women.
Choice D Reason: A 50% increase in maternal blood volume during pregnancy. This is an incorrect answer that describes a normal physiological change that occurs during pregnancy, not a cause of supine hypotensive syndrome. A 50% increase in maternal blood volume during pregnancy is due to increased production of plasma and red blood cells, which helps meet the increased oxygen and nutrient demands of the fetus and placenta, and prepares the mother for blood loss during delivery. A 50% increase in maternal blood volume during pregnancy does not cause hypotension or dizziness in pregnant women.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today