Why is it important for the nurse to assess the bladder regularly and encourage the laboring client to void every 2 hours?
Select one:
Frequent voiding encourages sphincter control.
A full bladder impedes oxygen flow to the fetus.
Frequent voiding prevents bruising of the bladder.
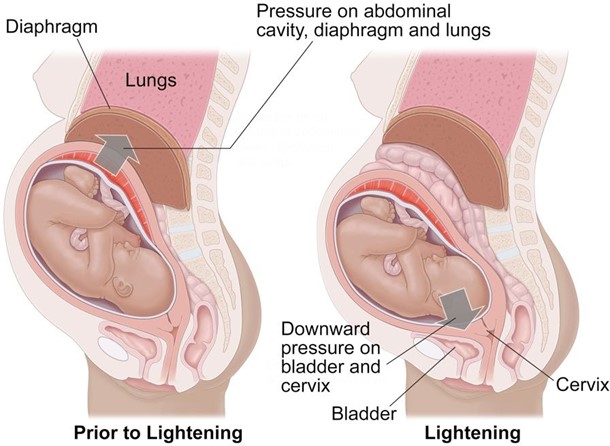
A full bladder can impede fetal descent.
The Correct Answer is D
Choice A Reason: Frequent voiding encourages sphincter control. This is an incorrect statement that has no relevance to labor and delivery. Sphincter control refers to the ability to contract and relax the muscles that control urination and defecation. It is not affected by frequent voiding.
Choice B Reason: A full bladder impedes oxygen flow to the fetus. This is an incorrect statement that confuses a full bladder with a prolapsed cord. A prolapsed cord is a condition where the umbilical cord slips through the cervix before the baby and becomes compressed by the fetal head, which can reduce oxygen flow to the fetus. A full bladder does not affect oxygen flow to the fetus.
Choice C Reason: Frequent voiding prevents bruising of the bladder. This is an incorrect statement that exaggerates the effect of a full bladder on the bladder wall. A full bladder may cause some pressure or discomfort on the bladder, but it does not cause bruising or damage.
Choice D Reason: A full bladder can impede fetal descent. This is a correct statement that explains why it is important for the nurse to assess the bladder regularly and encourage the laboring client to void every 2 hours.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: The cheek of the newborn is touched, and the newborn turns toward the side that was touched. This is an incorrect answer that describes a different reflex called the rooting reflex. The rooting reflex is a feeding reflex that helps the newborn locate the nipple and initiate sucking. The rooting reflex is elicited by stroking the cheek or corner of the mouth of the newborn, which causes them to turn their head and open their mouth toward the stimulus.
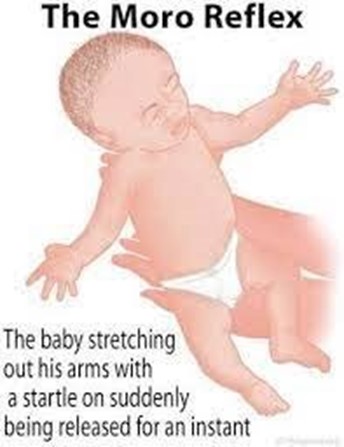
Choice B Reason: The newborn is suddenly lowered or startled, and they extend their arms, legs and neck, then rapidly bring their arms together. This is because this response describes the Moro reflex, which is a primitive reflex that is present at birth and disappears by 3 to 6 months of age. The Moro reflex is elicited by simulating a falling sensation or a loud noise, which triggers a fear response in the newborn. The Moro reflex consists of four phases: extension, abduction, adduction, and crying.
Choice C Reason: The newborn is supine and their head is turned to one side, then the arm on that same side extends. This is an incorrect answer that refers to another reflex called the tonic neck reflex. The tonic neck reflex is a postural reflex that helps prepare the newborn for voluntary reaching. The tonic neck reflex is elicited by placing the newborn in a supine position and turning their head to one side, which causes them to assume a "fencing" posture with one arm extended and one arm flexed.
Choice D Reason: The lateral aspect of the sole of the newborn's foot is stroked, and the toes extend and fan outward. This is an incorrect answer that indicates a different reflex called the Babinski reflex. The Babinski reflex is a neurological reflex that tests for spinal cord integrity. The Babinski reflex is elicited by stroking the lateral aspect of the sole of the foot from heel to toe, which causes the big toe to dorsiflex and the other toes to fan out.
Correct Answer is D
Explanation
Choice A Reason: Moderate amounts of deep red lochia. This is not a finding that would warrant further investigation, but rather a normal finding for the early postpartum period. Lochia is the vaginal discharge that occurs after delivery, which consists of blood, mucus, and tissue from the uterus. Lochia is usually deep red in color and moderate in amount for the first few days after delivery.
Choice B Reason: Sweating while afebrile. This is not a finding that would warrant further investigation, but rather a common occurrence in the postpartum period. Sweating is a mechanism of thermoregulation that helps the body eliminate excess fluid and electrolytes that were retained during pregnancy. Sweating does not necessarily indicate fever or infection.
Choice C Reason: Voiding 350 mL of blood-tinged urine. This is not a finding that would warrant further investigation, but rather an expected outcome for the postpartum period. Voiding large amounts of urine is normal in the postpartum period, as the body eliminates the excess fluid that was accumulated during pregnancy. Blood-tinged urine may be due to trauma or irritation of the urinary tract during labor or delivery, which usually resolves within a few days.
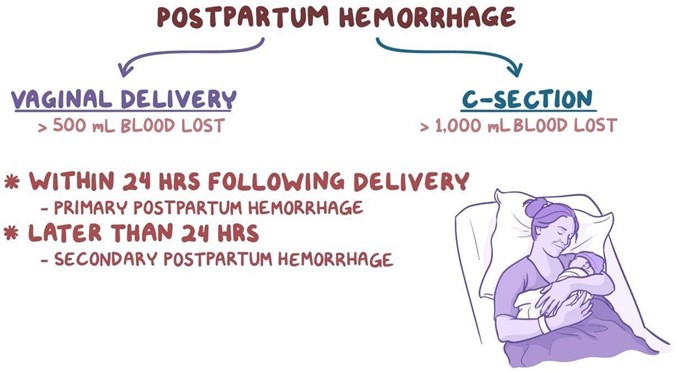
Choice D Reason: Heart rate of 115 beats/minute. This is because a heart rate of 115 beats/minute is higher than the normal range for an adult, which is 60 to 100 beats/minute. A high heart rate may indicate postpartum hemorrhage, infection, pain, anxiety, or dehydration. The nurse should further assess the client for other signs and symptoms of these conditions and notify the physician if necessary.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today